Microdosing GLP-1 for Autoimmune Conditions — What the Science Actually Says
Nobody told Fleming the mold on his petri dish would one day save two hundred million lives. He just looked carefully at what was in front of him.
That’s how medicine moves, when it moves honestly. A molecule is discovered for one purpose. Researchers look carefully. They find it doing other things — unexpected things, useful things. The anti-TNF biologics were developed for rheumatoid arthritis. Within a decade, they were reshaping treatment for Crohn’s disease, psoriasis, ankylosing spondylitis. Not because someone planned it that way. Because biology doesn’t read the original indication.
GLP-1 receptor agonists are on that same road.
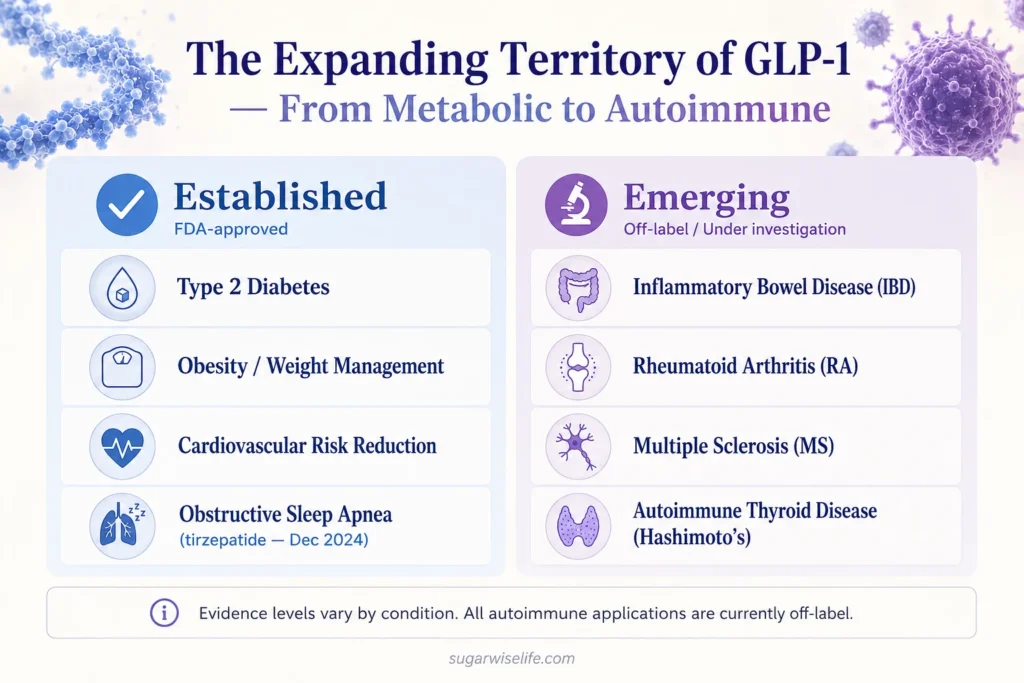
Approved for type 2 diabetes, then for obesity, then for cardiovascular protection — and now, at the edges of clinical practice, patients and clinicians are asking a different question: what if microdosing GLP-1 for autoimmune conditions could do something useful here too?
It’s a fair question. And it deserves a careful answer — not hype, not dismissal.
Table of Contents
How GLP-1 Works on Inflammation — The Mechanism That Started the Conversation
Before the question of autoimmune disease makes sense, the underlying biology needs to be clear.
GLP-1 receptors are not confined to the pancreas and gut. They are expressed in immune cells — including macrophages, T cells, and dendritic cells — and in the central nervous system, where neuroinflammation plays a role in a surprising range of conditions. When a GLP-1 receptor agonist binds these receptors, it doesn’t just regulate blood sugar. It modulates inflammatory signaling — specifically, it suppresses NF-κB activation and reduces pro-inflammatory cytokines including TNF-α, IL-6, and IL-1β.
This is not a side effect. It’s a direct pharmacological action.
A 2024 literature review by Alharbi, published in Therapeutic Advances in Endocrinology and Metabolism with 208 citations, characterized GLP-1 receptor agonists as having substantial anti-inflammatory effects with broad clinical implications in various diseases. The mechanism is real. What remains under investigation is how far that mechanism can be clinically leveraged — and at what dose.
For the full picture of how GLP-1 medications work, including their metabolic mechanisms, the complete guide covers that in detail.
What “Microdosing” Actually Means Here
The word microdosing carries precision in some contexts — in pharmacology, it refers to sub-pharmacological doses used to study drug behavior without therapeutic effect. In the GLP-1 and autoimmune conversation, it means something different and more informal: using GLP-1 medications at doses lower than standard obesity or diabetes protocols, specifically to target inflammatory pathways rather than weight loss.
There is no standardized microdosing protocol for GLP-1 in autoimmune conditions. No FDA-approved indication exists beyond obesity, type 2 diabetes, cardiovascular risk reduction, and — as of December 2024 — obstructive sleep apnea (tirzepatide only). Every use in autoimmune conditions is currently off-label.
That doesn’t make it wrong. It makes it a frontier. And frontiers require honesty about what we know, what we’re beginning to see, and what we’re still guessing at.
Is Microdosing GLP-1 for Autoimmune Conditions Legitimate?
The short answer is: the biological rationale is legitimate. The clinical evidence is early. The practice is ahead of the data.
That’s not unusual in medicine — it’s actually how most expansions in drug use begin. Anti-TNF biologics were used off-label in IBD for years before the RCT data caught up and formal approvals followed. The pattern is familiar to anyone who has watched a class of molecules mature.
Where GLP-1 sits today in the autoimmune space is roughly where anti-TNF agents were in the late 1990s: compelling mechanism, early observational signals, no definitive head-to-head trials, and a patient population that is not waiting for the science to finish moving before asking their doctors.
Condition by Condition — What the Data Actually Shows
Inflammatory Bowel Disease (IBD)
This is where the evidence is strongest outside of metabolic indications.
A 2024 observational study by Desai et al., published in Alimentary Pharmacology & Therapeutics, found that GLP-1 receptor agonist use in patients with type 2 diabetes was associated with a significantly lower risk of IBD-related surgery in patients with both ulcerative colitis and Crohn’s disease. This is not a randomized trial — confounding factors exist, and the population had diabetes as a comorbidity. But the signal is consistent with the known anti-inflammatory mechanism, and it has held across multiple analyses.
The gut, in some ways, is where GLP-1 was always most at home.
Rheumatoid Arthritis (RA)
A 2025 study by Kellner et al., published in ACR Open Rheumatology, examined the effect of GLP-1 receptor agonists in patients with rheumatoid arthritis who were overweight or obese. The findings showed improvement in RA disease activity scores alongside an improved cardiovascular risk profile.
The caveat matters here: the weight loss itself reduces systemic inflammation. Separating the direct anti-inflammatory effect of GLP-1 from the downstream effect of fat loss is methodologically difficult. The clinical benefit appears real. The mechanism attribution is still being untangled.
Multiple Sclerosis (MS)
A 2024 narrative review by Kaye et al. in Cureus examined the role of GLP-1 agonists in multiple sclerosis. The review found promising signals for both neuroprotective and anti-inflammatory effects — including potential improvement in nerve regeneration and reduction in central nervous system inflammation.
MS represents a different biological territory: the blood-brain barrier, central immune privilege, and a distinct pattern of autoimmune attack. The preliminary signals are interesting. The clinical evidence base is thin. This is the frontier of the frontier.
Autoimmune Thyroid Disease (Hashimoto’s)
This requires particular care, because two distinct conversations are happening simultaneously — and conflating them creates confusion.
The first conversation: GLP-1 receptor agonists carry an FDA black box warning regarding medullary thyroid carcinoma (MTC), based on rodent data. This is a cancer signal in a specific thyroid cell type, and it applies particularly to patients with a personal or family history of MTC or Multiple Endocrine Neoplasia type 2. The long-term side effect profile of GLP-1 medications addresses this warning in full.
The second conversation is entirely different: autoimmune thyroid disease, primarily Hashimoto’s thyroiditis, involves immune-mediated inflammation of thyroid tissue — a different mechanism, a different cell type, a different clinical question.
A 2025 literature review by Mazza, published in Cureus, found that GLP-1 receptor agonists showed potential in reducing inflammation and improving thyroid function specifically in patients with autoimmune thyroid disease and metabolic disorders. This is a distinct and cautiously encouraging signal — not to be conflated with the MTC warning.
The FDA warning does not preclude exploring GLP-1’s role in Hashimoto’s. It requires appropriate patient selection and informed discussion with a prescriber.
Which GLP-1 Medication, and at What Dose?
There is no evidence-based answer to this question specific to autoimmune conditions.
In clinical practice, when GLP-1 use in autoimmune patients is discussed, the same medications available for metabolic indications — primarily semaglutide and tirzepatide — are used at lower, often starter doses, sometimes maintained there rather than titrated upward. The rationale: capture the anti-inflammatory effect without the degree of appetite suppression and GI side effects that come with full therapeutic dosing for weight loss.
Whether this approach is more effective than standard dosing, or whether it achieves anything that standard dosing wouldn’t, has not been studied in controlled trials for any autoimmune indication.
For a clinical comparison of semaglutide and tirzepatide, including their mechanism differences and cardiovascular profiles, that comparison is covered in detail here.
The Conversation to Have With Your Doctor
If you have an autoimmune condition and are interested in whether GLP-1 therapy — at any dose — might be relevant for you, the conversation starts with your prescriber. Here is a framework for that discussion:
What to bring: Your current autoimmune diagnosis, your current medications (particularly immunosuppressants — potential interactions exist), your metabolic status (BMI, fasting glucose, lipid panel), and your understanding that this is off-label use in a space where evidence is early.
What to ask: Whether any trials are enrolling for your specific condition. Whether the anti-inflammatory rationale is applicable to your disease phenotype. Whether your specialist would be willing to co-manage with an endocrinologist or obesity medicine physician.
What to expect: A careful prescriber will be honest about the limits of current evidence. That’s not a door closing — it’s the beginning of a real clinical conversation.
Frequently Asked Questions
Can microdosing GLP-1 reduce inflammation?
GLP-1 receptor agonists have established anti-inflammatory effects through direct action on immune cells and inflammatory signaling pathways, including suppression of TNF-α, IL-6, and IL-1β. Whether sub-therapeutic “microdoses” produce meaningful anti-inflammatory effects independently of weight loss has not been studied in controlled trials.
Can you take GLP-1 with an autoimmune disease?
There is no blanket contraindication to GLP-1 use in autoimmune conditions. The main contraindications are a personal or family history of medullary thyroid carcinoma or MEN2, active pancreatitis, and pregnancy. Patients on immunosuppressive therapy should discuss potential interactions with their prescriber before starting any GLP-1 medication.
Can I take tirzepatide if I have an autoimmune disease?
Tirzepatide (Mounjaro/Zepbound) is not contraindicated in autoimmune conditions generally. As with all GLP-1 receptor agonists, standard contraindications apply, and use in autoimmune conditions specifically is currently off-label. The conversation with a prescriber is essential — particularly for patients on biologics or other immunomodulating therapies.
What is a microdose of tirzepatide for inflammation?
There is no standardized microdose protocol for tirzepatide in autoimmune or inflammatory conditions. In practice, some clinicians maintain patients at starter doses (2.5mg weekly) rather than titrating to the standard therapeutic range for weight loss. This approach has not been validated in clinical trials for any autoimmune indication.
Conclusion
The wheel didn’t know it would become civilization.
Neither did the mold on Fleming’s petri dish. Neither did the first rheumatologist who tried an anti-TNF biologic in a Crohn’s patient and watched something unexpected happen.
GLP-1 receptor agonists are not finished becoming what they are. The metabolic story is well-told. The autoimmune chapter is being written — carefully, in peer-reviewed journals, by researchers who are looking at the mechanism and following where it leads.
What the current science says is this: the biological rationale is real, the early signals in IBD and RA are promising, the MS and Hashimoto’s data is preliminary but not dismissible. And the practice of microdosing GLP-1 for autoimmune conditions, while ahead of the formal evidence, is not without logic.
Be rigorous. Be curious. Have the conversation with a physician who will do both.
— Dr. Nathan Wells, MD
Physician | 25+ years in clinical and pharmaceutical medicine
Take good care.
References
- Alharbi S. Anti-inflammatory role of glucagon-like peptide 1 receptor agonists and its clinical implications. Therapeutic Advances in Endocrinology and Metabolism. 2024.
- Desai A et al. Use of glucagon-like peptide-1 receptor agonists for type 2 diabetes mellitus and outcomes of inflammatory bowel disease. Alimentary Pharmacology & Therapeutics. 2024.
- Kaye A et al. The role of glucagon-like peptide-1 agonists in the treatment of multiple sclerosis: a narrative review. Cureus. 2024.
- Mazza AD. The thyroid twist: how GLP-1 agonists are influencing autoimmune thyroid care. Cureus. 2025.
- Kellner DA et al. Effect of glucagon-like peptide 1 receptor agonists on patients with rheumatoid arthritis. ACR Open Rheumatology. 2025.
Want practical metabolic health insights, weekly? No noise — just evidence-based clarity from a physician. → Subscribe to the SugarWiseLife weekly briefing
This article is for informational purposes only and does not constitute medical advice. The content on SugarWiseLife.com is intended to support, not replace, the relationship between you and your healthcare provider. Dr. Nathan Wells is a pen name used for privacy purposes. Nothing in this article should be used to diagnose or treat a medical condition. Always consult a qualified healthcare professional before making changes to your diet, exercise routine, or medication.





