GLP-1 Medications: The Complete Guide for Non-Diabetics
GLP-1 Non diabetic. If these two words feel like they don’t belong in the same sentence — that reaction is exactly why you’re here. For years, they didn’t.
GLP-1 medications were diabetes drugs. Full stop. Ozempic was for blood sugar. Semaglutide was for A1C. If you weren’t diabetic, the conversation wasn’t for you — and most physicians didn’t have it.
That equation has changed. The indication has expanded, the evidence has accumulated, and the question “can a non-diabetic take GLP-1?” is now one of the most searched medical queries in the US. Not because people are confused — because they’re paying attention.
I’ve been in medicine for over 25 years. I’ve watched medications get oversold and unfairly dismissed — often by the same industry cycle, just at different points of the curve. GLP-1 receptor agonists are no exception.
A medication isn’t a lifestyle accessory. You don’t start one because your friend lost twenty pounds and looked radiant at the reunion. But you also don’t dismiss one because the conversation got too loud, too commercial, too exhausting to follow.
I remember when asthmatic patients refused their inhalers — not because the science was wrong, but because dependency felt like weakness. We know how that story ended.
This guide isn’t about trend. It’s about whether this class of medications makes clinical sense for you — and what that actually means.
In This Guide
What Are GLP-1 Medications?
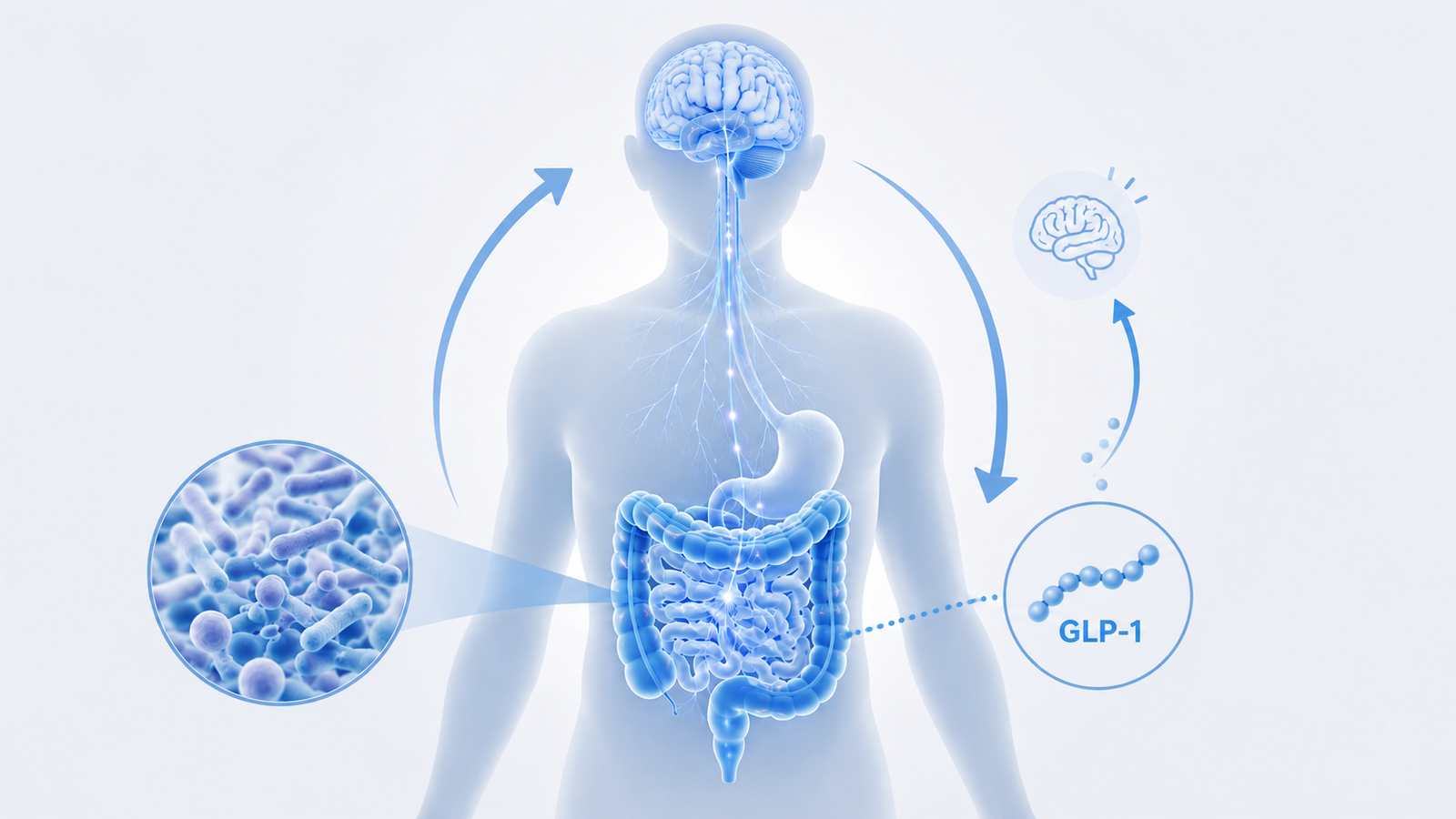
GLP-1 stands for glucagon-like peptide-1 — a hormone your gut naturally produces after eating. Its job: signal the pancreas to release insulin, slow gastric emptying, and tell the brain you’re full.
GLP-1 receptor agonists are synthetic molecules engineered to bind the same receptors with far greater potency and a much longer half-life. Where natural GLP-1 clears your system in minutes, semaglutide remains active for a full week. That difference isn’t trivial — it’s what makes the pharmacological effect sustained rather than fleeting.
The downstream effects are multiple and interconnected. Blood sugar regulation: insulin release is glucose-dependent, which means these medications don’t cause hypoglycemia in someone with a functioning pancreas — there is no crash. Gastric emptying: food leaves the stomach more slowly. You feel full sooner. You stay full longer. This isn’t a side effect; it’s the mechanism.
Then there’s what many patients notice first: the quieting of food noise. The background mental pull toward eating — the 3pm craving, the reflexive reach for something after dinner — fades significantly for most people on therapeutic doses. This is not willpower. It is pharmacology acting on hypothalamic GLP-1 receptors, shifting the neurological baseline your appetite operates from.
Beyond appetite, emerging data points to direct anti-inflammatory effects on the vasculature — independent of weight loss. This may partly explain why cardiovascular benefits appear in trials even before significant weight has been lost. The mechanism runs deeper than the scale.
What the Science Actually Says
The evidence base for GLP-1 non diabetic use is now built on three independent meta-analyses, not one sponsored trial.
Three independent meta-analyses, published over three consecutive years, tell a consistent story.
In 2022, Iqbal et al. (Obesity Reviews, 140+ citations) established the baseline: GLP-1 RAs produce significant weight reduction and glycemic improvements in overweight and obese adults without diabetes. The primary barrier to adherence was gastrointestinal — not cardiovascular or metabolic safety.
In 2023, Ansari et al. (Endocrine Practice) extended the picture. Beyond weight, GLP-1 RAs significantly improved blood pressure, lipids, and inflammatory markers in non-diabetic individuals. The cardiovascular signal was positive — not neutral.
In 2025, Moiz et al. (Annals of Internal Medicine) brought the analysis into the era of dual agonists, including tirzepatide. Same conclusion: robust efficacy on weight and cardiometabolic risk. Safety profile dominated by digestive side effects — manageable, not dangerous.
Three independent groups. Three consecutive years. Same conclusion. That kind of convergence is what earns a clinical recommendation.
Who Is a Candidate for GLP-1 as a Non Diabetic?
This is the question most guides skip, or answer with a liability-driven non-answer. Let me be direct.
The FDA has defined the approved indication: adults with a BMI ≥ 30, or BMI ≥ 27 with at least one weight-related comorbidity — hypertension, dyslipidemia, obstructive sleep apnea, or established cardiovascular disease. This covers both Wegovy (semaglutide) and Zepbound (tirzepatide) for chronic weight management in non-diabetic adults.
Strong candidates. Adults with BMI ≥ 30 who have not achieved durable weight loss with lifestyle modification alone — not because they lack motivation, but because the data on lifestyle-only interventions at this BMI shows a high relapse rate regardless of initial success. Adults with insulin resistance or prediabetes without a formal diabetes diagnosis. GLP-1 RAs slow the progression from prediabetes to type 2 diabetes — this is clinically meaningful, not incidental. Adults with metabolic syndrome — the cluster of abdominal obesity, hypertension, dyslipidemia, and impaired fasting glucose. GLP-1 RAs address multiple components simultaneously.
Women with PCOS or perimenopausal hormonal shifts are particularly likely to benefit from this evaluation.
Moderate candidates. Adults with BMI 27–30, no formal comorbidities, but significant metabolic risk based on family history, HOMA-IR elevation, or lipid panel. The evidence base thins here, but the clinical conversation is legitimate and worth having.
Poor candidates or absolute contraindications. Personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia type 2 — this is a hard stop, not a soft warning. Active or severe prior pancreatitis. Pregnancy or breastfeeding: not because harm is demonstrated, but because adequate safety data simply does not exist. Restrictive eating disorder history: appetite suppression in this context requires dedicated psychiatric assessment before any pharmacological intervention is considered.
Candidacy is not a checklist you complete alone. But knowing where you fall gives you the language to have the right conversation with a physician — and the confidence to push back if the conversation is dismissed without clinical reasoning.
If phentermine has come up in that conversation, here’s how it compares to GLP-1 medications.
Which GLP-1 Is Best for Weight Loss in a Non Diabetic?
Tirzepatide (Zepbound) currently shows the highest average weight loss in trials — 15–20% of body weight, driven by its dual GLP-1/GIP mechanism. Semaglutide (Wegovy) has the longer safety record and stronger cardiovascular evidence base.
The honest answer: the best GLP-1 is the one you can access, tolerate, and sustain. A medication that is 20% more effective in a trial and discontinued at week 8 due to cost or side effects is not the better clinical choice for you.
For a detailed breakdown of how semaglutide and tirzepatide compare — mechanism, trial data, cost, and a clinical framework to choose between them — see: [Semaglutide vs Tirzepatide — What the Data Actually Shows].
What Happens If a Non Diabetic Takes GLP-1?
In a non-diabetic adult, appetite drops, gastric emptying slows, and food noise quiets — often within the first two weeks. Weight loss follows, at a rate that depends heavily on dose, diet quality, and activity. Blood sugar doesn’t crash — the mechanism is glucose-dependent.
The timeline of effects, dose escalation, and what to monitor week by week deserves its own dedicated guide.
Side Effects: What to Know Before You Start
Nausea, slowed digestion, occasional vomiting — real, dose-related, and for most patients time-limited. The discontinuation rate due to GI side effects in major trials is 7–10%. More than 90% complete the protocol.
Constipation is one of the most common GI complaints on GLP-1 medications — predictable, manageable, and covered in full here.
Some signals — thyroid risk, pancreatitis — have been handled sensationally. The data in human populations tells a more reassuring story. The cardiovascular signal runs consistently in the other direction: favorable.
For a full breakdown of what the long-term data actually shows — including the one effect that requires active management — see GLP-1 Long-Term Side Effects — Proven Facts.
One side effect that doesn’t always make the clinical handout: hair shedding. It occurs in a meaningful subset of patients, typically peaking between months four and six, and is in most cases reversible. The mechanism is more nuanced than it appears — and so is the response. GLP-1 and hair loss: what’s actually driving it and what you can do
This is why supervised use isn’t a constraint — it’s your best clinical asset.
What About Muscle and Bone?
Any significant weight loss — caloric restriction, bariatric surgery, or pharmacotherapy — carries a risk of lean mass reduction. GLP-1-induced weight loss is not exempt from this.
Clinical trial data suggests that roughly 25–40% of weight lost on semaglutide or tirzepatide may come from lean mass, in the absence of structured resistance training. This is comparable to other weight loss interventions — not worse. But it is not zero, and it matters.
The clinical implication is straightforward: if you’re initiating a GLP-1 receptor agonist for weight management, structured resistance training is not optional. Not yoga. Not walking. Progressive resistance — the kind that creates mechanical load on muscle tissue and forces adaptation. This is the only intervention with consistent evidence for lean mass preservation during pharmacological weight loss.
Protein intake matters equally. Maintaining 1.2–1.6g per kilogram of bodyweight daily is the current evidence-based recommendation during active weight loss — particularly when appetite suppression reduces total food volume. You are eating less; you need to eat better.
On bone density: the data is less mature, but some studies suggest modest reductions in bone mineral density with significant GLP-1-induced weight loss, particularly in older adults. For patients over 60 or with pre-existing osteopenia, this warrants proactive monitoring — a DEXA scan at baseline is a reasonable clinical ask.
The medication creates a metabolic opportunity. What you do with that opportunity determines whether you emerge leaner and stronger, or simply lighter.
The Brain Effect: A Signal Worth Watching
GLP-1 receptors exist in the brain — in the hypothalamus and beyond. This is established neuroanatomy. Emerging data suggests GLP-1 RAs may reduce neuroinflammation and exert neuroprotective effects. Trials for semaglutide in Alzheimer’s disease are ongoing.
That neurological footprint extends into sleep itself — enough to earn tirzepatide a sleep apnea — a separate FDA approval, independent of its metabolic indications.
The “food noise” reduction most patients describe — the quiet that descends on their relationship with eating — may reflect direct brain activity, not merely a secondary consequence of weight loss.
This is a promising signal. Don’t start a GLP-1 medication for cognitive health. Do follow this space.
⚠️ GLP-1 Supplements Are Not GLP-1 Medications
Products marketed as “GLP-1 boosters” or “natural semaglutide alternatives” are supplements — not pharmaceuticals. They do not bind GLP-1 receptors. They are not regulated for efficacy.
Berberine has legitimate metabolic data — modest improvements in insulin sensitivity and lipid profiles. It is not “nature’s Ozempic.” That framing collapses the mechanistic difference between a supplement that mildly influences a pathway and a molecule engineered to activate a specific receptor with clinical precision.
The distinction matters clinically and financially. Spending $50/month on a product that doesn’t work is not a safer version of a medication that does.
The Moral Panic Around GLP-1
There is a recurring anxiety in the public conversation that has nothing to do with pharmacology. It sounds like this: “Isn’t this cheating?” “What happened to willpower?” “Are people just taking the easy way out?”
I want to address this directly — because it reaches the exam room and affects real clinical decisions.
Obesity and insulin resistance are not character failures. They are metabolic states shaped by genetics, hormonal biology, environment, the food supply, sleep, and chronic stress. When we ask whether someone “deserves” pharmacological help with weight, we don’t ask the same question about antihypertensives, statins, or thyroid medications. The inconsistency is not medicine. It is stigma.
At the same time — and this nuance matters — a GLP-1 medication initiated without lifestyle context, resistance training, and nutritional attention is a significantly less effective intervention than one embedded in a coherent metabolic approach. The medication amplifies what you give it to work with. It doesn’t replace it.
Not cheating. Not a shortcut. A clinical tool — like every other clinical tool — that works best when the patient is an active participant, not a passive recipient.
How to Access GLP-1 Without a Diabetes Diagnosis
Three pathways exist: traditional physician referral, telehealth platform, or — in limited circumstances — a 503A compounding pharmacy with prescriber documentation.
What you actually pay depends almost entirely on your insurance status, the savings programs you know about, and the pharmacy you choose. For a full pricing breakdown across every access route, see The Cheapest Way to Get GLP-1 — All Your Options.
Frequently Asked Questions
What happens if a non-diabetic takes GLP-1?
In a non-diabetic adult, GLP-1 receptor agonists reduce appetite, slow gastric emptying, and produce meaningful weight loss — without causing hypoglycemia. Insulin release is glucose-dependent, so blood sugar doesn’t crash in someone with a functioning pancreas. The most striking early effect for many patients is a sharp reduction in food cravings and the mental pull toward eating.
Which GLP-1 is best for weight loss without diabetes?
Tirzepatide (Zepbound) currently shows the highest average weight loss in trials — around 15–20% of body weight. Semaglutide (Wegovy) has a longer safety record and stronger cardiovascular data. The best choice is the one you can access, tolerate, and sustain. A drug discontinued at week 8 due to cost or side effects is not the better clinical option.
Who cannot take GLP-1 medications?
Absolute contraindications include a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia type 2. Pregnancy and breastfeeding are also contraindicated. Active or prior severe pancreatitis warrants caution. A history of restrictive eating disorders requires psychiatric assessment before initiating any appetite-suppressing pharmacotherapy.
How long to lose 20 pounds on GLP-1?
Timelines vary significantly by starting weight, dose, diet quality, and activity. In major trials, 15–20% body weight loss occurred over 68–72 weeks at full therapeutic dose. For a 180-pound person, 20 pounds represents roughly 11% — achievable within 20–30 weeks for many participants, though individual response varies considerably.
Can you get GLP-1 for weight loss without a prescription?
No. GLP-1 receptor agonists require a prescription from a licensed clinician. Telehealth platforms offer legitimate prescription pathways with clinical oversight. Products marketed as “GLP-1 boosters” are supplements — they do not bind GLP-1 receptors and are not regulated for efficacy the way pharmaceuticals are.
How to Have an Honest Conversation With Your Doctor
Not sure if you have insulin resistance? Start with a structured self-assessment before your appointment.
“My BMI is [X], I have [comorbidity or metabolic risk], I’ve pursued lifestyle changes consistently, and I’d like to discuss whether a GLP-1 receptor agonist is appropriate — and what monitoring you’d want in place.”
That framing opens a clinical conversation, not a demand. If it’s dismissed without reasoning, a second opinion from a metabolic medicine specialist is appropriate.

— Dr. Nathan Wells, MD
Physician | 25+ years in clinical and pharmaceutical medicine
Take good care.
Want practical metabolic health insights, weekly? Get your free physician’s guide — “5 Signs You Have Insulin Resistance” — plus evidence-based clarity from a physician, straight to your inbox. → Subscribe to the SugarWiseLife weekly briefing
This article is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. GLP-1 receptor agonists are prescription medications — their use should be evaluated and supervised by a qualified healthcare provider familiar with your complete medical history. Always consult your physician before starting, stopping, or changing any medication.
For full details, see our Medical Disclaimer, Editorial Policy, and Affiliate Disclosure.