GLP-1 for Sleep Apnea — What the Data Shows
There’s a conversation that happens in clinics every day. A patient walks out with a new diagnosis — obstructive sleep apnea — and a physician who means well delivers one of two sentences.
The first: Lose weight. Which is both medically accurate and spectacularly unhelpful as a standalone prescription. The patient nods, already knowing, already failing.
The second: You’ll need a CPAP. A machine with a name that sounds like a military acronym. A mask. A hose. A companion for every night of the rest of their life. The patient drives home grey and quiet.
For some, there was a third option — surgery. Which is its own kind of sentence.
A third door has been opening quietly since December 2024: GLP-1 for sleep apnea. For the first time, a medication — not a device, not a scalpel — carries an FDA indication specifically for this condition. The data behind it deserves an honest read.
In this article
What Obstructive Sleep Apnea Actually Does to You
Obstructive sleep apnea is not simply loud snoring. It is a nightly cycle of partial or complete airway collapse — the soft tissue at the back of the throat relaxing to the point where airflow stops.
The clinical measure is the apnea-hypopnea index, or AHI: the number of these breathing disruptions per hour of sleep. The “4% rule” you may have seen referenced reflects the standard diagnostic threshold — an event counts when airflow drops by 30% or more and oxygen saturation falls by at least 4%.
The severity classification:
- Mild: 5–14 events/hour
- Moderate: 15–29 events/hour
- Severe: ≥30 events/hour
Each event is a micro-arousal. The brain pulls the body back from the edge of apnea. The patient never reaches the deeper stages of restorative sleep. Over months and years, this translates to elevated blood pressure, metabolic dysregulation, impaired glucose control, and a cardiovascular risk profile that compounds quietly.
OSA and metabolic syndrome share more than a waiting room. They accelerate each other. A patient with insulin resistance who sleeps poorly becomes more insulin resistant. The cycle tightens.
Why Weight Is the Upstream Problem
The airway is a tube held open by muscle tone. In the supine position — lying flat — gravity pulls the tongue, soft palate, and lateral pharyngeal walls inward. In most people, muscle tone compensates. In OSA, it doesn’t.
Excess fat tissue around the neck and pharynx narrows the tube before it ever has a chance to collapse. The critical measurement is neck circumference, not body weight alone — but the two are related. A 10% reduction in body weight reduces AHI by approximately 26%, according to observational data. The airway widens. The collapse threshold rises.
This is not a moral argument. It is anatomy. The airway doesn’t care why the tissue is there — it responds to its absence.
What makes weight-focused treatment difficult has always been the weight loss itself. Telling a patient with severe OSA, poor sleep quality, and metabolic dysregulation to “just lose weight” ignores the physiological cascade working against them. Sleep deprivation impairs leptin and ghrelin regulation. Fatigue reduces physical activity. Insulin resistance makes caloric partitioning less efficient.
The upstream problem is real. What was missing was an upstream lever powerful enough to pull.
How GLP-1 Medications Work on Sleep Apnea
GLP-1 receptor agonists act on sleep apnea through at least two mechanisms — one well-established, one emerging.
The primary mechanism is weight loss. Tirzepatide and semaglutide produce the most significant sustained weight reduction of any pharmacological option available. As adipose tissue around the pharynx decreases, airway patency improves. This is not a GLP-1-specific effect — it is weight loss acting on anatomy. What GLP-1 medications contribute is the depth and durability of the reduction.
The secondary mechanism is direct anti-inflammatory and potentially neuromodulatory action. GLP-1 receptors are present in airway tissue, and early data suggests that GLP-1 agonists may improve upper airway muscle tone beyond what weight loss alone would predict. The evidence here is preliminary. Researchers are still parsing how much of the AHI improvement in trials is weight-mediated versus receptor-mediated. The honest answer, for now, is: mostly weight, possibly more.
That distinction matters less clinically than it does scientifically. For the patient, the result is the same — and the result is meaningful.
What SURMOUNT-OSA Actually Showed
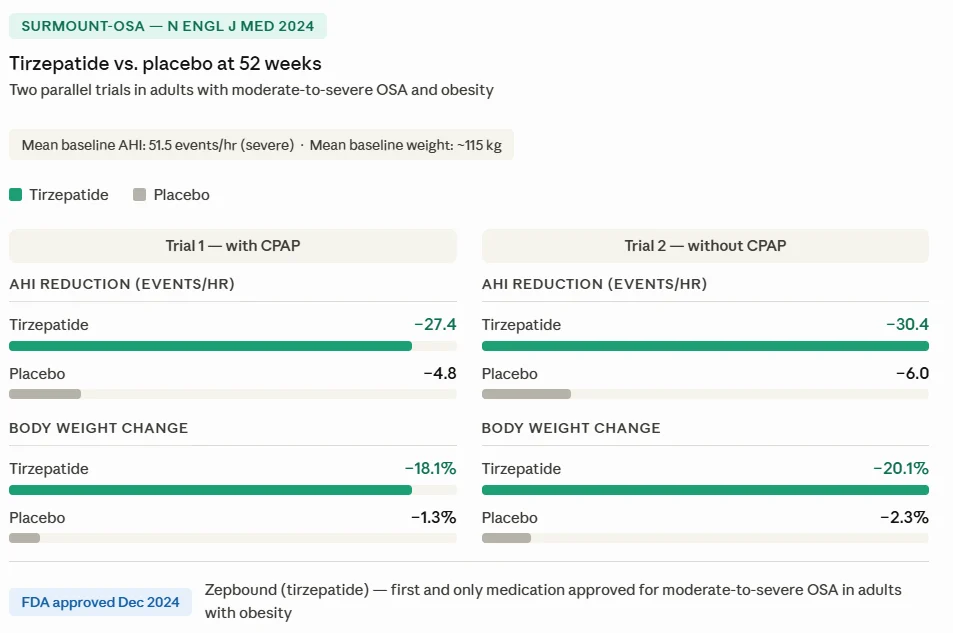
SURMOUNT-OSA was a Phase 3 program — two parallel randomized controlled trials — testing tirzepatide specifically in adults with moderate-to-severe obstructive sleep apnea and obesity. Published in the New England Journal of Medicine in 2024 (Malhotra et al.), it is the pivotal trial behind the FDA approval.
The two arms addressed different clinical realities: Trial 1 enrolled patients who were using CPAP; Trial 2 enrolled patients who were not. The mean AHI at baseline was 51.5 events per hour in both trials — well into the severe range.
The results at 52 weeks:
- AHI reduction: −27.4 events/hour in Trial 1, −30.4 in Trial 2 — versus −4.8 and −6.0 with placebo
- Body weight: −18.1% in Trial 1, −20.1% in Trial 2 — versus approximately −1.3% and −2.3% with placebo
- Systolic blood pressure: clinically meaningful reductions in both arms
To put the AHI numbers in clinical terms: a patient entering with 51.5 events per hour — severe — ends the trial at approximately 21–24 events per hour. Still moderate. But no longer severe. Not resolved. Meaningfully reduced.
The FDA approved Zepbound (tirzepatide) for moderate-to-severe OSA in adults with obesity in December 2024 — making it the first and only medication with this specific indication.
Two independent meta-analyses published in 2025 — Altobaishat et al. in the European Clinical Respiratory Journal and Aljazeeri et al. in the American Journal of Respiratory and Critical Care Medicine — confirmed the signal across GLP-1 receptor agonists as a class: significant AHI reduction, weight loss, and blood pressure improvement. A 2024 scoping review by Le et al. noted that long-term durability data remain limited. A fair caveat.
Which GLP-1 Is FDA-Approved — and Which Aren’t
This matters more than it might seem, because it shapes insurance coverage, prescribing pathways, and the language your physician will use.
Zepbound (tirzepatide): FDA-approved for moderate-to-severe OSA in adults with obesity. The only GLP-1 receptor agonist with this specific indication. Approval added December 2024.
Wegovy (semaglutide): FDA-approved for chronic weight management and cardiovascular risk reduction. Not approved for OSA as a specific indication.
Ozempic (semaglutide): FDA-approved for type 2 diabetes and cardiovascular risk reduction. Not approved for OSA.
Semaglutide does have positive data on sleep apnea outcomes — the meta-analyses cited above include semaglutide studies. But a data signal and an FDA indication are different things. A physician can prescribe semaglutide off-label for a patient with OSA; they cannot bill that prescription against an OSA indication.
FDA indications evolve. The regulatory landscape described here reflects December 2024 — and new data can shift what is approved, for which molecule, and under what conditions. Your prescriber will have the most current picture.
The practical implication: if insurance coverage for GLP-1 therapy on the basis of your OSA diagnosis is part of your conversation, Zepbound is the only option with that pathway open. For a full breakdown of coverage options and costs, see our dedicated guide.
What This Means for Your CPAP
This is where the clinical nuance matters most — and where oversimplification does real harm.
GLP-1 medications are not CPAP killers. They are not designed to eliminate the device from your life. Whether they do depends on your individual anatomy, the severity of your OSA at baseline, and how much of your airway obstruction is weight-mediated versus structural.
Two profiles emerge clinically:
The patient who tolerates CPAP poorly
The mask leaks, the pressure is claustrophobic, the compliance data shows four hours of use on a good night. For this patient, significant weight loss may raise the threshold above which their airway collapses on its own. With physician reassessment — a repeat sleep study — some patients reach a point where the CPAP becomes genuinely superfluous. Not all. Not most. But some.
The patient who has learned to live with CPAP
Good compliance, good sleep quality, CPAP integrated into daily life. For this patient, GLP-1-mediated weight loss may allow pressure titration downward, improve overall sleep architecture, and reduce the metabolic burden that OSA was creating. The device may not disappear — but its role may diminish.
The goal is not to avoid what is necessary. It is to reduce dependence on what becomes superfluous. Those are different conversations, and they belong at different moments in treatment.
Do not stop using CPAP on the basis of weight loss alone without a clinical reassessment. The airway is not visible from the outside.
For a full picture of what to expect over time on GLP-1 therapy, see GLP-1 Long-Term Side Effects — Proven Facts.
Who Is a Good Candidate
The FDA-approved indication is specific: moderate-to-severe obstructive sleep apnea in adults with obesity (BMI ≥30). This is the population SURMOUNT-OSA enrolled and the population for whom we have robust data.
Outside this profile:
Mild OSA (AHI 5–14): No approved indication. The data does not support a formal recommendation. Some physicians may consider it in the context of broader metabolic management — but this is off-label, and the risk-benefit conversation looks different.
OSA without obesity: The mechanism is primarily weight-mediated. Without significant excess adipose tissue contributing to airway obstruction, the expected benefit is lower.
Diabetes not required. The approval is weight- and OSA-specific. A patient without diabetes, without cardiovascular disease, but with moderate-to-severe OSA and a BMI above 30 falls squarely within the indication.
If you are on CPAP and have not discussed GLP-1 therapy with your prescriber, this is a conversation worth initiating — with your sleep medicine physician or primary care provider, not instead of them.
For a broader overview of who qualifies for GLP-1 medications, see GLP-1 Medications: The Complete Guide for Non-Diabetics.
Frequently Asked Questions
Which GLP-1 is FDA-approved for sleep apnea?
Zepbound (tirzepatide) is the only GLP-1 receptor agonist with an FDA indication specifically for obstructive sleep apnea. The approval, added in December 2024, covers moderate-to-severe OSA in adults with obesity. Semaglutide (Wegovy, Ozempic) has supporting data but carries no OSA-specific FDA approval.
What is the 4% rule for sleep apnea?
The 4% rule refers to the oxygen desaturation criterion used in AHI scoring. A breathing event is counted when airflow drops by 30% or more and blood oxygen falls by at least 4%. This threshold defines what qualifies as a clinically significant apnea or hypopnea in standard diagnostic protocols.
Does insurance cover GLP-1 for sleep apnea?
Coverage varies by plan. Zepbound’s FDA approval for OSA creates a legitimate coverage pathway that did not exist before December 2024, but prior authorization requirements still apply. Medicare, Medicaid, and employer plans handle this differently. See our full breakdown of GLP-1 coverage options and costs.
Can GLP-1 replace CPAP?
For some patients, significant weight loss under GLP-1 therapy may reduce OSA severity enough that CPAP becomes superfluous — confirmed by a repeat sleep study. For others, it reduces device dependence without eliminating it. GLP-1 is not designed to replace CPAP; it addresses an upstream driver. Clinical reassessment determines what that means for each patient.
Conclusion
The door that opened in December 2024 is not wide open for everyone. It has a frame — moderate-to-severe OSA, obesity, and a prescriber willing to have the conversation. But it exists.
That matters.
For years, the tools we had required patients to change before we could help them. Now one of the tools helps with the change itself. The sentence is no longer the only option.
— Dr. Nathan Wells, MD
Physician | 25+ years in clinical and pharmaceutical medicine
Take good care.
References
- Malhotra A, Grunstein RR, Fietze I, et al.; SURMOUNT-OSA Investigators. Tirzepatide for the Treatment of Obstructive Sleep Apnea and Obesity.
- Altobaishat O et al. Safety and Efficacy of Glucagon-Like Peptide-1 Receptor Agonists in Patients with Obstructive Sleep Apnea: A Systematic Review and Meta-Analysis. European Clinical Respiratory Journal. 2025.
- Aljazeeri J et al. GLP-1 Receptor Agonists for Obstructive Sleep Apnea: A Meta-Analysis of Randomized Controlled Trials. Am J Respir Crit Care Med. 2025.
- Le KDR et al. The Impact of Glucagon-Like Peptide-1 Receptor Agonists on Obstructive Sleep Apnoea: A Scoping Review. Pharmacy. 2024.
Want practical metabolic health insights, weekly? No noise — just evidence-based clarity from a physician. → Subscribe to the SugarWiseLife weekly briefing.
This article is for informational purposes only and does not constitute medical advice. The content on SugarWiseLife.com is intended to support, not replace, the relationship between you and your healthcare provider. Dr. Nathan Wells is a pen name used for privacy purposes. Nothing in this article should be used to diagnose or treat a medical condition. Always consult a qualified healthcare professional before making changes to your diet, exercise routine, or medication.