How Long Does GLP-1 Take to Work? A Real-World Timeline
If you’ve started a GLP-1 medication and watching the scale every morning or just wondering how long does GLP-1 take to work, this article is for you..
The pharmacology is actually quite predictable. GLP-1 receptor agonists — semaglutide, tirzepatide, liraglutide — have well-documented kinetics. Peak plasma levels. Dose titration windows. Measurable appetite changes within specific timeframes. The science is clear.
What isn’t predictable is what you do during that window.
I’ve seen patients start a GLP-1 and describe it as a turning point — the first time eating felt manageable. I’ve also seen patients on the same medication, at the same dose, say it “did nothing.” In almost every case, the difference wasn’t the drug.
This article gives you the real timeline: what GLP-1 does, when it does it, and what that actually means for your results.
In This Article
First, a distinction worth making
“Working” means two different things when it comes to GLP-1 therapy — and conflating them is the source of most frustration.
It’s a distinction I’ve encountered throughout my years with clinical research: lab activity and clinical relevance are not the same thing. A molecule can be doing exactly what it’s designed to do — and the patient in front of you can feel nothing yet. Both things are true at once.
There’s pharmacological activity — the drug binding to receptors, slowing gastric emptying, signaling satiety to the brain. This happens within hours of your first dose. The molecule is doing its job almost immediately.
Then there’s clinical results — measurable weight loss, reduced appetite, improved metabolic markers. This takes weeks. Sometimes months. And it’s dose-dependent: most patients don’t reach their therapeutic dose until week 12 or later, because GLP-1 medications require gradual titration to minimize side effects.
Expecting visible results in week two is like expecting a full harvest in the week after planting. The biology is working. The timeline is just longer than most people expect.
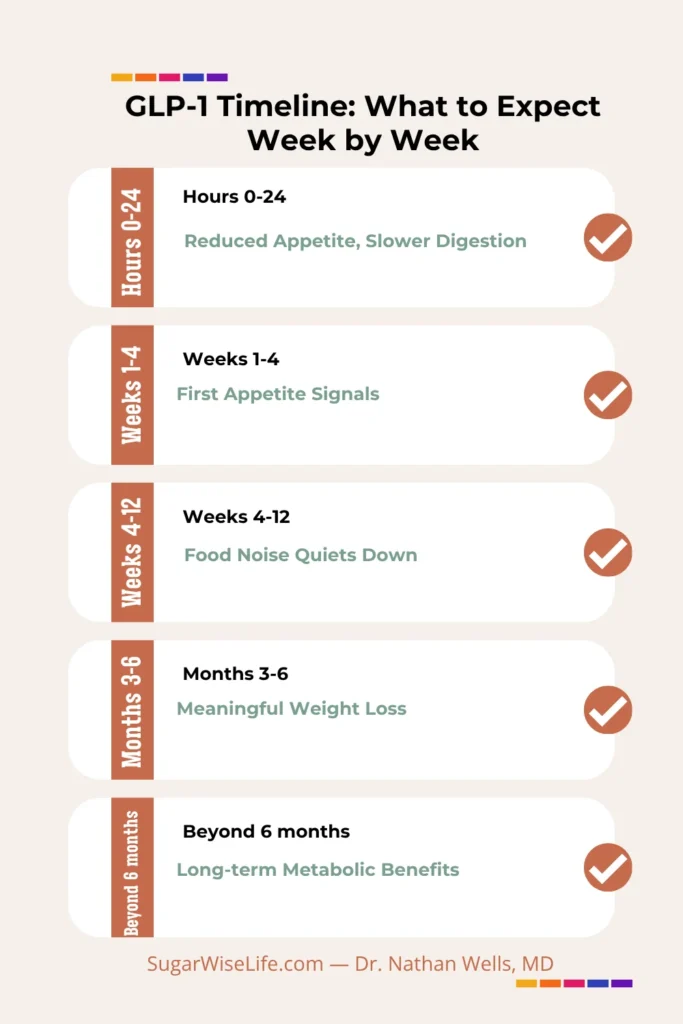
The GLP-1 timeline, week by week
Hours 0 to 24: Pharmacological onset
GLP-1 receptor agonists reach peak plasma concentration within hours of injection, depending on the formulation. Semaglutide (Ozempic/Wegovy), injected once weekly, peaks between 24 and 72 hours post-injection. Some patients notice a mild reduction in appetite within the first 24 hours. Most don’t feel anything significant yet — and that’s entirely normal.
GI side effects, if they’re going to occur, often start in this window. Nausea is the most common early signal. It’s the dose doing exactly what it’s supposed to do — slowing gastric emptying — at a dose your gut hasn’t calibrated to yet. For a closer look at what persists beyond the early months, see GLP-1 Long-Term Side Effects — Proven Facts.
Weeks 1 to 4: Building the foundation
The first month is typically the lowest effective dose — below what most patients need for meaningful weight loss. Think of it as a tolerance-building phase, not a results phase.
Appetite changes are subtle at this stage. Some patients report earlier fullness. Some notice they’ve stopped thinking about food between meals. Some notice nothing at all.
This is also when many patients worry. “It’s not working.” It is. You’re just not at the therapeutic dose yet.
GI side effects — including constipation — tend to peak during dose escalation. If constipation is your main concern, the full management protocol is here
Weeks 4 to 12: First real signal
Most titration schedules reach a meaningful dose somewhere between month one and month three. This is when appetite suppression becomes more consistent — less food noise, smaller portions feeling satisfying, reduced cravings for high-calorie foods.
A 2021 review in Advances in Therapy (Ard et al.) found that GLP-1 receptor agonists produce significant and sustained weight reduction in obese patients, with effects becoming clinically meaningful in this window. Weight loss of 1–2% of body weight per month is a reasonable early benchmark.
Months 3 to 6: The productive window
By month three, most patients are at or near their target dose. Weight loss continues, but the pace varies significantly based on diet, activity level, and metabolic baseline.
A 2025 meta-analysis (Guo et al.) found that GLP-1 RAs show varying efficacy profiles across this period, with the most significant weight reduction seen in patients who paired medication with behavioral changes.
Beyond 6 months: Long-term trajectory
A 2025 systematic review (Li et al.) noted that while GLP-1 RAs produce persistent improvement in glycemic control and weight loss, some weakening of effects can occur after two years. This doesn’t mean the medication stops working — it means the body adapts, and dose adjustment or lifestyle recalibration may be needed.
How long does GLP-1 take to suppress appetite?
Most patients notice the first signs of appetite suppression within the first one to two weeks — earlier fullness, less urgency to eat, reduced interest in snacking. But this is at the starter dose, which is deliberately low.
Consistent, meaningful appetite suppression — what patients describe as food noise going quiet — typically appears between weeks four and eight, once the dose has been titrated upward.
Semaglutide’s half-life of approximately one week means the drug accumulates over multiple doses before reaching steady-state plasma levels. This is partly why appetite effects deepen over time rather than appearing all at once.
If you’ve been on a GLP-1 for two weeks and feel nothing, you’re likely still in the foundation phase. Give the titration schedule time to do its job.
For a complete overview of GLP-1 medications and how they work, see: GLP-1 Medications: The Complete Guide for Non-Diabetics.
How do you know if GLP-1 is working?
The scale isn’t always the most sensitive early indicator. Here are the signs that often precede measurable weight loss by several weeks:
- You finish meals with food still on your plate
- You forget to eat, or realize lunch passed without urgency
- Food you used to crave feels less compelling
- You feel satisfied on smaller portions
- The mental preoccupation with food — food noise — has quieted
These are pharmacological responses to GLP-1 receptor activation. If none of them are present by week eight at a meaningful dose, that’s worth discussing with your prescribing physician.
One note: some patients respond better to tirzepatide than semaglutide, because tirzepatide also targets GIP receptors. If one agent isn’t producing appetite changes at therapeutic dose, a different formulation may be worth exploring — not a different approach entirely.
Why GLP-1 might not seem to be working
Let’s address the most common reasons — plainly.
You’re still in the titration phase
The starting dose of most GLP-1 medications is not the therapeutic dose. Ozempic starts at 0.25 mg weekly, Mounjaro at 2.5 mg — a dose designed for tolerance, not weight loss. Expecting clinical results at 0.25 mg is a mismatch of expectations, not a failure of the medication.
You’re eating around it
GLP-1 reduces appetite. It doesn’t override appetite. Patients who use the reduced hunger window to eat differently — more protein, less processed food, smaller portions — see results. Patients who compensate with calorie-dense foods often don’t. The medication creates space. What you do with that space is yours to decide. And that detail matters more than most people realize.
You’re measuring the wrong thing
Weight fluctuates by two to four pounds daily based on hydration, sodium, and bowel transit. Week-to-week scale readings are noise. Month-to-month trends are signal. If you’re weighing yourself every morning and drawing conclusions, you’re watching static.
The dose isn’t optimized yet
Not everyone responds equally to the same dose. Some patients need a higher dose to achieve meaningful appetite suppression. This is a normal part of GLP-1 therapy — not a failure.
If you are weighing whether to switch from semaglutide to tirzepatide, the full clinical framework is here: Semaglutide vs Tirzepatide — What the Data Actually Shows — before having a talk with your doctor.
Does GLP-1 work without diet changes?
Technically, yes. GLP-1 receptor agonists produce weight loss even without deliberate dietary changes — the appetite suppression itself leads to spontaneous caloric reduction in most patients.
But “technically yes” and “clinically meaningful” are not the same thing.
The studies showing 15% to 20% body weight loss were conducted alongside lifestyle counseling. Real-world results without any behavioral engagement tend to be more modest and less durable.
There’s a pattern I’ve seen consistently in practice. The patient who approaches GLP-1 as a tool — something to work with, not something to hand the work to — tends to compound the results. The medication quiets food noise. They use that quiet to build better habits. Those habits outlast the medication.
The patient who deposits the problem and waits for the medication to return results? The medication often eventually returns to the pharmacy.
GLP-1 is a partner. Not a delegate.
How long should you give GLP-1 to work?
The clinical benchmark is a minimum of 16 weeks at therapeutic dose before drawing conclusions about efficacy.
That’s not 16 weeks from the first injection. That’s 16 weeks after reaching the maintenance dose — which itself takes 8 to 12 weeks to reach on standard titration schedules.
In practical terms: most clinicians assess meaningful efficacy around months five to six from initiation.
Stopping during the titration phase — when side effects are most prominent and results are minimal — is the most common reason GLP-1 therapy appears to fail. It’s not the medication failing. It’s an incomplete trial.
If you’re at month four, at therapeutic dose, with no appetite change, no weight movement, and no quality-of-life improvement — that’s a legitimate signal to bring to your physician. That’s not quitting early. That’s a real data point.
Frequently Asked Questions
How long does GLP-1 take to work to suppress appetite?
Initial appetite suppression can appear within the first one to two weeks, but consistent effects — what patients describe as food noise quieting — typically emerge between weeks four and eight, once the dose has been titrated to a therapeutic level. Semaglutide’s weekly accumulation means effects deepen over successive doses.
How do I know if GLP-1 is working?
Early signs include finishing meals with food remaining, reduced urgency to eat between meals, and decreased preoccupation with food (food noise). These often appear before significant weight loss. Measurable weight reduction typically becomes visible by weeks eight to twelve at therapeutic dose.
Why is GLP-1 not working for me?
The most common reasons: you’re still in the titration phase (starting doses are not therapeutic doses), you’re measuring too early, the dose hasn’t been optimized, or caloric compensation is offsetting appetite suppression. If you’re at therapeutic dose with no response after 16 weeks, discuss formulation alternatives with your physician.
Does GLP-1 work without diet changes?
GLP-1 produces some weight loss even without deliberate diet changes, through spontaneous caloric reduction. But the most significant and durable results in clinical trials occurred alongside lifestyle engagement. The medication reduces appetite — what you do with that reduced appetite determines how far the results go.
How long should I give GLP-1 to work?
The standard clinical benchmark is 16 weeks at therapeutic dose. Since titration itself takes 8 to 12 weeks, most clinicians evaluate meaningful efficacy around months five to six from the first injection. Stopping during the titration phase is the most common reason GLP-1 therapy appears to fail.
The Bottom Line
The timeline is pharmacological. The results are personal.
GLP-1 gives you a quieter relationship with food — and with yourself. The noise steps back. You take the wheel again, decide the direction, breathe. And discover, maybe for the first time in a while, that there are other things worth savoring. and something else becomes possible.
What you build in that window is the part that’s yours.
— Dr. Nathan Wells, MD
Physician | 25+ years in clinical and pharmaceutical medicine
Take good care.
Want practical metabolic health insights, weekly? No noise — just evidence-based clarity from a physician. → Subscribe to the SugarWiseLife weekly briefing
This article is for informational purposes only and does not constitute medical advice. The content on SugarWiseLife.com is intended to support, not replace, the relationship between you and your healthcare provider. Dr. Nathan Wells is a pen name used for privacy purposes. Nothing in this article should be used to diagnose or treat a medical condition. Always consult a qualified healthcare professional before making changes to your diet, exercise routine, or medication.