Is Phentermine a GLP-1? What You Need to Know
The question makes sense. Both suppress your appetite. Both appear in weight loss conversations. Both get prescribed in doctors’ offices. So when someone asks: ” is phentermine a GLP-1 medication”, they’re not confused — they’re just working with incomplete information.
Here’s the short answer: no. Phentermine is not a GLP-1 medication. Not even close.
But the longer answer is where it gets interesting — because understanding the difference doesn’t just settle a vocabulary question. It helps you understand what your body is actually being asked to do when you take either one.
Table of Contents
No — And the Difference Runs Deeper Than You Think
Phentermine belongs to a class of drugs called sympathomimetic amines. It works by stimulating your central nervous system — specifically by triggering the release of norepinephrine in the brain, which suppresses appetite through a fight-or-flight type signal. Think of it as turning up the urgency dial in your nervous system until food stops feeling like a priority.
GLP-1 receptor agonists — semaglutide (Ozempic, Wegovy), tirzepatide (Mounjaro, Zepbound) — work through an entirely different pathway. GLP-1 stands for glucagon-like peptide-1, a hormone your gut naturally produces after eating. GLP-1 medications mimic this hormone, slowing gastric emptying, reducing appetite through receptors in the hypothalamus, and quieting what researchers call “food noise” — the constant mental preoccupation with eating that many people with obesity describe as relentless.
One drug mimics a stress response. The other mimics a satiety hormone. Same outcome on the scale. Completely different conversations with your body.
How Phentermine Actually Works
Phentermine was FDA-approved in 1959 — making it the oldest weight loss medication still commonly prescribed in the United States. That longevity is part of why it’s so entrenched in clinical practice. Generations of physicians trained on it.
Mechanistically, phentermine triggers the release of norepinephrine — and to a lesser extent dopamine and serotonin — in the hypothalamus. This activates the sympathetic nervous system, the same system that responds to perceived danger. Hunger becomes a lower priority. Energy expenditure increases modestly. Appetite drops.
It works. In the short term.
The issue is durability. The FDA’s labeling recommends phentermine for short-term use only — typically no more than 12 weeks — because tolerance develops and cardiovascular effects accumulate over time. It is a Schedule IV controlled substance under the DEA — a classification formalized in 1973 — in the same regulatory category as benzodiazepines. That classification reflects its dependency and misuse potential.
Phentermine is sold under brand names including Adipex-P and Lomaira. It is also available in combination with topiramate (an anticonvulsant with independent appetite-suppressing effects) under the brand name Qsymia, which received FDA approval in 2012. Neither phentermine nor topiramate is a GLP-1 medication — Qsymia works through entirely different pathways.
To the question that comes up often — what organ is phentermine hard on? — the honest answer is the heart. Phentermine raises heart rate and blood pressure. It is contraindicated in patients with cardiovascular disease, uncontrolled hypertension, hyperthyroidism, and a history of drug abuse. The ghost of fen-phen — the 1990s combination of fenfluramine and phentermine, withdrawn after cardiac valve damage was documented — still shapes how cautiously many cardiologists approach it today. Worth noting: the FDA did not withdraw phentermine. It was fenfluramine that left the market. Fenfluramine has since returned under a different name (Fintepla, approved 2020) for a different indication — pediatric epilepsy — at doses far below those used for weight loss. Phentermine never went anywhere.
How GLP-1 Medications Work — The Short Version
GLP-1 receptor agonists mimic a hormone your intestine secretes in response to food. They slow the passage of food from your stomach, reduce appetite signals in the brain, and lower the background preoccupation with eating that many patients describe as constant and exhausting.
They are not controlled substances. They have no stimulant properties. And unlike phentermine, they carry documented long-term cardiometabolic benefits — including a 20% reduction in major cardiovascular events in the SELECT trial, the largest cardiovascular outcomes study in obesity medicine to date.
For a full breakdown of how GLP-1 medications work, who they’re appropriate for, and what the evidence base looks like, see the complete guide to GLP-1 medications for non-diabetics.
Phentermine vs GLP-1 — A Clinical Side-by-Side
These two medication classes address the same problem through mechanisms so different they belong to different eras of medicine. The comparison below covers what clinicians and patients actually want to know.
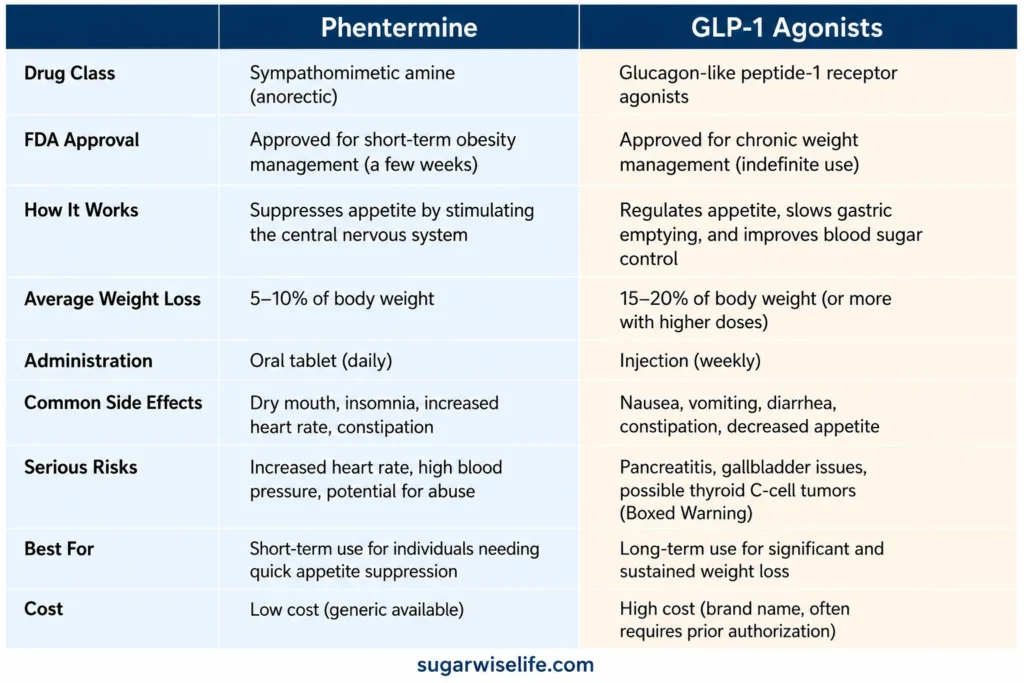
The cost gap is real and worth addressing directly. Phentermine is cheap — often $30–60 per month as a generic. GLP-1 medications at branded prices exceed $1,000 per month. Access options, savings programs, and telehealth pathways are covered in full in the guide to the cheapest way to get GLP-1 medications.
For a detailed comparison of semaglutide and tirzepatide specifically, see: Semaglutide vs Tirzepatide — What the Data Actually Shows.
Can You Take Phentermine and a GLP-1 Together?
This question surfaces regularly in telehealth consultations and online forums — and it deserves a straight answer.
Some physicians do prescribe phentermine alongside a GLP-1 medication, typically in patients who are not losing weight at the expected rate and have no cardiovascular contraindications. The rationale: add a short-term appetite suppressant while the GLP-1 dose is still titrating up toward its therapeutic level.
In practice, there is no randomized controlled trial evaluating this combination for safety or efficacy. What exists is off-label clinical experience and a small number of observational reports.
The cardiovascular concern is real. Phentermine raises heart rate and blood pressure. GLP-1 medications can also modestly affect heart rate during initiation. Combining two agents that influence cardiovascular parameters — without robust trial data — warrants careful patient selection and close monitoring.
If your prescriber is considering this combination, the right questions to ask: What is your baseline blood pressure and resting heart rate? What is the planned duration of phentermine in this protocol? What are the monitoring checkpoints?
This is not a combination to self-initiate.
Which Is Right for You?
Phentermine is not inferior to GLP-1 medications. It is different. It was designed for a different era of medicine, for a different model of what obesity is. In that model, obesity was a short-term problem requiring short-term suppression. Twelve weeks, lose the weight, move on.
What we now understand — and what the GLP-1 data has made undeniable — is that obesity is a chronic metabolic condition. Not a discipline problem. Not a willpower deficit. A condition with identifiable biological drivers that respond to long-term pharmacological management, the same way hypertension and dyslipidemia do.
That shifts the calculus significantly.
Phentermine may make sense for:
- Patients who cannot afford GLP-1 therapy
- Patients who need short-term support around a specific intervention or event
- Patients with no cardiovascular risk factors who want a defined, time-limited option
GLP-1 medications may make sense for:
- Patients seeking durable metabolic change
- Patients with insulin resistance, prediabetes, or metabolic syndrome
- Patients with established or elevated cardiovascular risk
- Patients for whom the long-term outcomes data matters
As for why doctors hesitate on phentermine: the Schedule IV classification adds prescribing friction. The fen-phen history created lasting liability caution. And physicians who now have access to GLP-1 medications increasingly find it difficult to justify a short-term stimulant when a long-term metabolic option exists — unless cost is the barrier. Cost, of course, is often the barrier.
Frequently Asked Questions
Is phentermine a GLP-1 medication?
No. Phentermine is a sympathomimetic amine that works by releasing norepinephrine in the brain to suppress appetite. GLP-1 medications mimic a gut hormone that regulates satiety through the gut-brain axis. They belong to entirely different drug classes with different mechanisms, different durations of use, and different safety profiles.
Is phentermine safer than semaglutide?
Neither is universally safer — it depends on the patient. Phentermine carries cardiovascular risks (elevated heart rate and blood pressure) that make it inappropriate for patients with heart disease or uncontrolled hypertension. Semaglutide has a documented cardiovascular benefit profile from the SELECT trial. For most patients with metabolic risk factors, the long-term safety data favors GLP-1 medications.
Why do doctors not like to prescribe phentermine?
Several reasons converge: it is a Schedule IV controlled substance requiring additional prescribing oversight, its cardiovascular profile limits use in higher-risk patients, it is recommended for short-term use only, and its association with fen-phen — withdrawn in 1997 after cardiac valve complications — created lasting caution. Physicians with access to GLP-1 options increasingly prefer the long-term data profile those medications offer.
Can you take phentermine with a GLP-1 together?
Some physicians prescribe this combination off-label, typically to bridge the titration phase of a GLP-1 medication. No randomized controlled trial has evaluated it formally. The main concern is additive cardiovascular effects — both agents can influence heart rate and blood pressure. This is a clinical decision requiring individual risk assessment, not a self-managed protocol.
The Bottom Line
Phentermine and GLP-1 medications both reduce appetite. That is where the similarity ends.
One was born in 1959, when obesity was treated like an acute inconvenience. The other emerged from decades of incretin research that reframed obesity as a chronic metabolic condition with identifiable hormonal drivers. Both have a role. Neither is for everyone.
The question was never really “is phentermine a GLP-1?” The question underneath it is: what is weight, what drives it, and what does it mean to treat it seriously? That question has a longer answer now — and a better one — than it did before.
— Dr. Nathan Wells, MD
Physician | 25+ years in clinical and pharmaceutical medicine
Take good care.
References
5. U.S. Food and Drug Administration. Phentermine hydrochloride — drug label and approval history. FDA.gov.
Want practical metabolic health insights, weekly? No noise — just evidence-based clarity from a physician. → Subscribe to the SugarWiseLife weekly briefing.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. The content on SugarWiseLife.com is intended to support, not replace, the relationship between you and your healthcare provider. Dr. Nathan Wells is a pen name used for privacy purposes. Nothing in this article should be used to diagnose or treat a medical condition. Always consult a qualified healthcare professional before making changes to your diet, exercise routine, or medication.