Semaglutide vs Tirzepatide — What the Data Actually Shows
Semaglutide vs tirzepatide — that is the question I encounter almost everywhere: in my talks, in my inbox, in the consulting room. “Doctor, which one should I ask for?” Sometimes it comes with a printout. Sometimes with a Reddit thread highlighted. Always with the same underlying hope: that one drug is simply better than the other, and that knowing which one will make the decision easy.
It won’t.
Not because the data is unclear — it isn’t, and we will go through all of it here. But because “better” is a word that belongs to populations, not patients. What clinical trials tell us about average weight loss across thousands of participants says nothing about what will happen in your body, with your metabolic profile, your insurance plan, your tolerance for side effects, and your life.
Semaglutide and tirzepatide are both genuine medical advances. They work differently, produce different average results, cost differently, and come with different real-world access realities. Understanding those differences is how you walk into that conversation with your doctor prepared. If you are new to this class of medications, the complete guide to GLP-1 medications is the right starting point before reading this comparison.
In This Article
One Extra Receptor — Why Tirzepatide Isn’t Just a Stronger Semaglutide
Both drugs belong to the GLP-1 class. If you have already read the complete guide to GLP-1 medications, you know how that mechanism works — the appetite signaling, the slowed gastric emptying, the glucose-dependent insulin release. That foundation applies to both drugs.
What makes tirzepatide different is not dose. It is target.
Semaglutide (Ozempic, Wegovy) is a GLP-1 receptor agonist. It activates one receptor type. Tirzepatide (Mounjaro, Zepbound) is a dual agonist — it activates both the GLP-1 receptor and the GIP receptor (glucose-dependent insulinotropic polypeptide).
GIP is the other incretin hormone. Historically, researchers were uncertain whether GIP agonism would meaningfully add to GLP-1 activity — in people with obesity, GIP receptor signaling appears blunted. The clinical surprise from tirzepatide’s program was that combining both pathways produced effects larger than either alone.
Why might GIP matter beyond weight loss? Current evidence points to several mechanisms: enhanced insulin secretion across a wider glucose range, possible direct effects on adipose tissue metabolism, and a signal relevant to lean mass preservation. The GIP receptor is expressed in skeletal muscle and bone tissue, and early data suggests the dual agonism may modestly attenuate lean mass loss. This remains an area of active research.
The practical implication: tirzepatide is not semaglutide at a higher dose. It works through a broader metabolic mechanism. That distinction shapes how we read the comparative data.
What the Head-to-Head Trial Actually Tells Us
For years, comparing these two drugs meant comparing separate trials — different populations, different protocols, different baselines. An indirect comparison that no rigorous clinician should use with confidence.
That changed with SURMOUNT-5, published in The New England Journal of Medicine in 2025. The first true head-to-head randomized controlled trial. Same eligibility criteria, same follow-up duration. Tirzepatide versus semaglutide, at maximum tolerated doses, over 72 weeks.
The results: participants on tirzepatide lost an average of 20.2% of their body weight. Participants on semaglutide lost 13.7%. A difference of approximately 6.5 percentage points — statistically significant and clinically meaningful.
Before drawing the obvious conclusion, three things deserve attention.
First: “maximum tolerated dose” is not “maximum labeled dose.” Many participants did not reach the highest dose tier. The comparison reflects whatever each individual tolerated — which introduces variability across the trial population.
Second: SURMOUNT-5 is the comparison that counts — not SURMOUNT-1 versus STEP-1. Those earlier trials used different run-in periods, different baseline characteristics, and different dosing timelines. Citing them as a head-to-head comparison, as many published articles still do, is methodologically incorrect.
Third: average outcomes mask individual variation. In every trial, there are participants who lose 5% and participants who lose 35%. The average tells you what is likely across a population, not what will happen to you.
The headline is real: tirzepatide outperforms semaglutide for weight reduction in the best available evidence. What that means for any individual patient is a separate, and more important, question.
Both remain a different class of treatment entirely from older appetite suppressants. For patients weighing these options against phentermine, the comparison starts here.
Semaglutide vs Tirzepatide for Weight Loss — By the Numbers
The table below puts the key clinical parameters side by side.
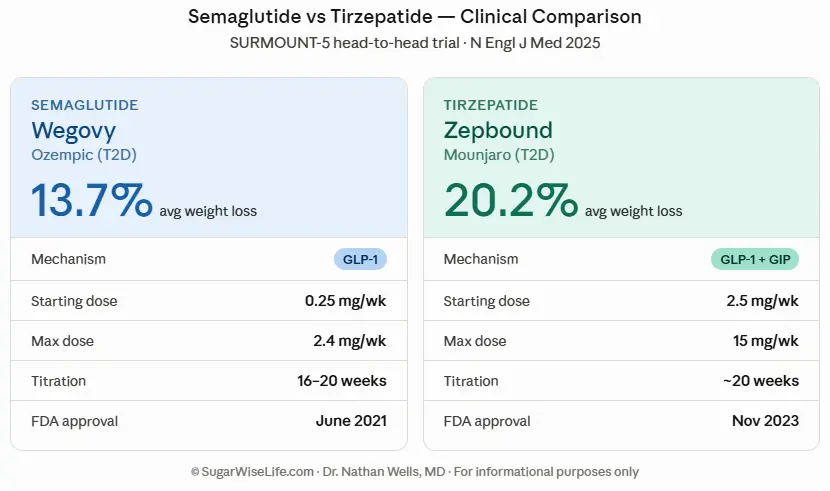
Weight loss data from SURMOUNT-5 (NEJM 2025) — adults with obesity without type 2 diabetes, at maximum tolerated dose over 72 weeks. Brand names differ by indication: Wegovy and Zepbound are FDA-approved for obesity; Ozempic and Mounjaro are approved for type 2 diabetes. The same molecule, a different regulatory context.
To put the weight loss figures in real terms: a person starting at 220 pounds would expect to lose approximately 30 pounds on semaglutide and 44 pounds on tirzepatide — at maximum tolerated dose, over 72 weeks, under clinical trial conditions. Real-world results vary, and individual response depends on metabolic profile, dose tolerance, and the lifestyle structure built around the medication.
Tirzepatide also carries an indication that semaglutide does not: it is FDA-approved for obstructive sleep apnea in adults with obesity — a clinically distinct advantage
for patients who present with both conditions.
One critical note: how quickly you progress through the titration schedule matters as much as which drug you take. For a detailed week-by-week breakdown of what to expect at each phase, see: How Long Does GLP-1 Take to Work?.
FDA indications evolve. The regulatory landscape described here can shift what is approved with new data, for which molecule, and under what conditions. Your prescriber will have the most current picture.
Do You Lose More Muscle on Semaglutide or Tirzepatide?
This is one of the most clinically important — and most underreported — questions in the GLP-1 conversation.
Both drugs cause lean mass loss. When people lose weight rapidly on GLP-1 medications, a meaningful portion of that weight comes from lean tissue rather than fat. Estimates from clinical trial body composition data range from 25 to 40 percent of total weight lost. That includes muscle — a real concern, particularly for older adults and anyone whose mobility, strength, or long-term metabolic function depends on preserving it.
Does tirzepatide do better on this metric? The honest answer: modestly, probably, based on early data. The GIP receptor is expressed in skeletal muscle and adipose tissue, and there is a biological rationale for tirzepatide having a slightly more favorable lean mass profile. Some analyses from the SURMOUNT program suggest a marginally lower proportion of lean mass loss compared to semaglutide at equivalent total weight reduction. But the data is not yet robust enough for a definitive clinical claim.
What is robust: the single biggest predictor of lean mass preservation on either drug is resistance training combined with adequate protein intake — at least 1.2 to 1.6 grams per kilogram of body weight per day. That recommendation applies equally regardless of which molecule you are taking.
The choice between semaglutide and tirzepatide will not save your muscle. Your training and nutrition habits will.
Side Effects — Where the Two Drugs Actually Differ
The side effect profiles of semaglutide and tirzepatide overlap substantially. Both cause primarily gastrointestinal effects — nausea, vomiting, diarrhea, constipation — especially during the titration phase. Both carry the same class warnings: a theoretical thyroid C-cell tumor signal observed in rodent models but not confirmed in humans, and a history of pancreatitis as a contraindication.
Nausea at initiation: Clinical experience and patient-reported data suggest tirzepatide may produce more pronounced nausea at the start of titration, possibly attributable to its dual receptor mechanism. This typically resolves within the first several weeks as the body adapts.
Long-term safety data: Semaglutide has been on the market longer. Its cardiovascular benefit data — established in the SELECT trial (2023), demonstrating a significant reduction in major cardiovascular events in adults with obesity without diabetes — is more mature than tirzepatide’s cardiovascular outcomes data, which is accumulating but more recent.
Individual tolerability: This is the variable that matters most in practice. Some patients tolerate tirzepatide better; others do significantly better on semaglutide. There is no reliable way to predict this in advance. Tolerability is discovered through experience, not selected through trial comparisons.
Neither drug is categorically safer. The risk-benefit calculation is individual.
Cost, Insurance, and What Really Determines Your Choice
Here is a clinical reality that rarely appears in comparison articles: for most patients, the prescribing decision is not made by the evidence. It is made by the insurance company.
List prices without coverage: Wegovy (semaglutide) runs approximately $1,349 per month. Zepbound (tirzepatide) runs approximately $1,059 per month. Eli Lilly launched Zepbound at a lower price point — a deliberate strategic decision. Both drugs remain unaffordable for most patients without insurance or manufacturer savings programs.
The compounding pharmacy question
For a period, patients accessed far cheaper compounded versions of both drugs through telehealth prescribing platforms. That window has narrowed significantly. The FDA removed tirzepatide from its drug shortage list in late 2024, determining that Eli Lilly could supply sufficient branded product to meet demand. This effectively ended the legal basis for compounding pharmacies to produce copies of tirzepatide. Semaglutide’s shortage designation has been more prolonged, but the regulatory environment is tightening here as well.
What this means clinically
The drug that your insurance covers at an affordable tier is, in most cases, the right drug to start with. If you have no coverage for either, manufacturer programs — Eli Lilly’s Zepbound Savings Card and Novo Nordisk’s NovoCare program — and telehealth platforms offering structured prescribing pathways are worth exploring before comparing mechanism and efficacy data.
If you are considering either medication and want guidance on which option is realistic for your situation, a telehealth provider specializing in metabolic health can review your clinical profile and help you navigate the access landscape.
Which One Is Right for You? A Clinical Framework
Not a verdict. A framework for the conversation with your prescriber.
Consider tirzepatide if:
- Your BMI is ≥35 and you need substantial weight reduction
- You have previously tried semaglutide at therapeutic dose for 16+ weeks and lost less than 5% of your starting weight
- You have type 2 diabetes alongside obesity — Mounjaro is FDA-approved for both indications
- Your insurance covers Zepbound or Mounjaro, or you qualify for Lilly’s savings card
Consider semaglutide if:
- Your insurance covers Wegovy or Ozempic but not Zepbound
- You have established cardiovascular disease — the SELECT trial data on semaglutide’s cardiovascular benefit is more developed
- You prefer the longer post-market safety track record
- Cost is a primary constraint and semaglutide has better coverage under your specific plan
The responder phenotype
Neither drug’s response is fully predictable. Some patients who show minimal response to semaglutide become strong responders when switched to tirzepatide — likely due to differences in GIP receptor sensitivity. The reverse is less common but documented.
The clinical benchmark: if you are at therapeutic dose — not still titrating — for 12 to 16 weeks and have lost less than 5% of your starting weight, the drug may not be the right fit. That is the moment to discuss switching with your physician, not after two weeks at the lowest starter dose.
The most important variable
No drug works in isolation. Both semaglutide and tirzepatide perform significantly better when combined with structured nutritional support, resistance training, and ongoing medical follow-up. The question “which one is right for you” is inseparable from the question “what support structure are you building around it?”
What’s Coming — Retatrutide and the Next Chapter
The semaglutide versus tirzepatide comparison is already taking place in the shadow of a third molecule. Retatrutide is a triple agonist — targeting GLP-1, GIP, and glucagon receptors simultaneously. Phase 3 trials are underway. Phase 2 data showed average weight loss approaching 24% of body weight over 48 weeks — exceeding what either currently approved drug achieves in the best head-to-head evidence available today.
What this means for patients considering these two drugs now: it is not a reason to wait. Retatrutide is not yet approved. The timeline to approval is measured in years, not months. The patients who benefit most from this class of medications are the ones who start treatment when they need it, with the best available option at that moment — not the ones waiting for the pipeline to mature.
This landscape is moving fast. But metabolic disease does not wait for the next approval cycle— and the expanding territory of GLP-1 into autoimmune conditions is the next chapter worth watching.
Frequently Asked Questions
Which one is better, semaglutide or tirzepatide?
In the only head-to-head trial published to date (SURMOUNT-5, NEJM 2025), tirzepatide produced greater average weight loss — approximately 20% versus 14% over 72 weeks. However, the right choice depends on your clinical profile, insurance coverage, individual tolerability, and response at therapeutic dose. Superior average trial results do not automatically translate to the best choice for a specific patient.
Do you lose more muscle on semaglutide or tirzepatide?
Both drugs cause lean mass loss, estimated at 25 to 40% of total weight lost. Tirzepatide may offer a modestly more favorable lean mass profile due to GIP receptor activity in skeletal muscle, but this is not yet conclusively established. The most effective strategy for preserving muscle on either drug is resistance training and adequate protein intake — at least 1.2 g/kg/day.
Why did the FDA remove tirzepatide from the shortage list?
The FDA declared the tirzepatide shortage resolved in late 2024, determining that Eli Lilly could supply sufficient quantities of Mounjaro and Zepbound to meet national demand. This effectively ended the legal basis for compounding pharmacies to produce tirzepatide copies — which many patients had been accessing at substantially lower cost. Patients on compounded tirzepatide were advised to transition to the commercial product.
How long does it take to lose 20 lbs on tirzepatide?
This depends on starting weight, dose tolerated, and individual response. A 20-pound loss for someone starting at 220 lbs represents roughly 9% of body weight — most tirzepatide responders reach this within 3 to 5 months at therapeutic dose. For a week-by-week breakdown of the full timeline, see: How Long Does GLP-1 Take to Work?.
Semaglutide vs Tirzepatide: The Bottom Line
he data on semaglutide vs tirzepatide is clear about what these drugs do in populations. It is silent about what they will do in you. That silence is not a failure of medicine — it is an honest description of how individual biology works.
What you can act on: understand the mechanism difference, know your insurance reality, build the right support structure around whichever drug you start, and agree with your prescriber in advance on what “working” looks like — and at what point you reassess.
The right drug is the one that moves your metabolic health forward. Everything else is detail.
— Dr. Nathan Wells, MD
Physician | 25+ years in clinical and pharmaceutical medicine
Take good care.
References
- Aronne LJ et al. Tirzepatide as Compared with Semaglutide for the Treatment of Obesity (SURMOUNT-5). N Engl J Med. 2025.
- Jastreboff AM et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). N Engl J Med. 2022;387(3):205–216.
- Wilding JPH et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity (STEP-1).
- Tan B et al. Efficacy and safety of tirzepatide for treatment of overweight or obesity: a systematic review and meta-analysis. International Journal of Obesity. 2023.
- Lincoff AM et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes (SELECT).
Want practical metabolic health insights, weekly? No noise — just evidence-based clarity from a physician. → Subscribe to the SugarWiseLife weekly briefing
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. The content on SugarWiseLife.com is intended to support, not replace, the relationship between you and your healthcare provider. Dr. Nathan Wells is a pen name used for privacy purposes. Nothing in this article should be used to diagnose or treat a medical condition. Always consult a qualified healthcare professional before making changes to your diet, exercise routine, or medication.