Insulin Resistance Test at Home + HOMA-IR Calculator
Before You Buy Anything, Read This
An insulin resistance test at home sounds simple, every week, patients come to me having already spent money on a test kit they don’t fully understand — or having convinced themselves they’re “fine” based on a number they misread.
The phrase “insulin resistance test at home” is everywhere right now. It’s also deeply misleading, because it means at least three completely different things depending on where you see it. A product listing on Amazon, a lab ordering page, and a clinical blog are all using the same four words to describe entirely different things.
My job here isn’t to steer you toward a purchase. It’s to give you the same clarity I give patients in my office: what can you actually measure, what does each method tell you, and what do your numbers mean once you have them.
If you’ve already had fasting bloodwork done in the past year, you may be able to calculate your insulin resistance status today — for free — without ordering a single new test. We’ll get to that.
In this article
The Problem: “At Home” Doesn’t Mean What You Think It Does
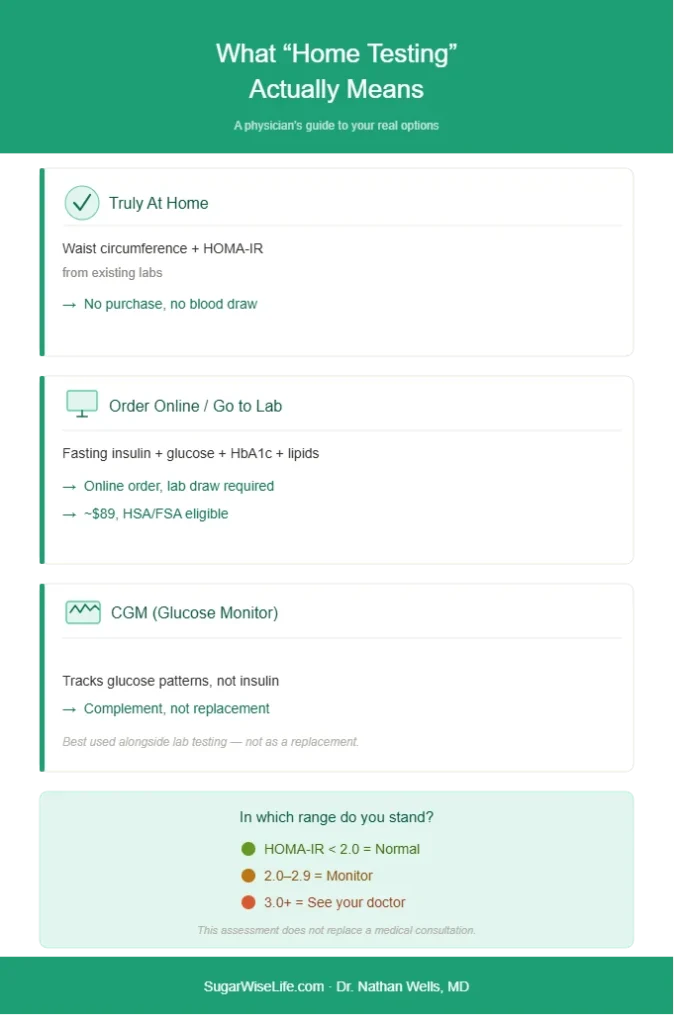
Before interpreting any number, you need to understand what category of test you’re dealing with. There are three, and they are not interchangeable.
Category 1 — Truly At Home (No Lab Required)
These methods require no purchase, no blood draw, no lab visit. You either already have the data you need, or you can obtain it with a tape measure.
Waist circumference measurement. This is the most underused and most underestimated screening tool in clinical practice. Central adiposity — specifically, excess fat around the abdominal organs — is both a cause and a consequence of insulin resistance. It doesn’t require a blood draw.
Measure at the level of your navel, relaxed, not pulled in. Elevated risk thresholds (these are widely accepted clinical reference points):
- Men: ≥ 40 inches (102 cm)
- Women: ≥ 35 inches (88 cm)
Note that these thresholds are calibrated for populations of European descent. South Asian, East Asian, and some Middle Eastern populations carry metabolic risk at lower waist measurements — a nuance most online guides ignore entirely.
Waist circumference won’t give you a precise metabolic score. But if you’re above the threshold and have other warning signs, it’s meaningful clinical information — and it costs nothing, they described in How to Tell If You Have Insulin Resistance .
HOMA-IR from your existing bloodwork. This is the most important point in this entire article, and it appears rarely on the web: if you already have a fasting glucose and a fasting insulin result from any recent blood panel, you can calculate your HOMA-IR right now.
Many patients have had these values measured without knowing it — as part of a routine metabolic panel, a pre-diabetes check, or a thyroid/hormonal workup. Check your patient portal or your lab report. If both values are there, scroll down to the calculator.
Category 2 — Order Online, Go to a Lab (Not Truly At Home)
This is the most commonly advertised category. Services like LabCorp, Healthlabs, and others allow you to order a test panel online without a physician’s prescription, then walk into a local draw center to give your blood sample. The result arrives digitally.
This is legitimate, convenient, and genuinely useful — but it is not a home test. You still need a venipuncture at a certified lab. The “home” part refers only to the ordering process.
What to know before you use one of these services:
Order a panel, not a single test. Fasting insulin alone, without fasting glucose, gives you incomplete information. You need both to calculate HOMA-IR — the most validated proxy for insulin resistance in epidemiological and clinical research. A good insulin resistance panel will include:
- Fasting insulin
- Fasting glucose
- HbA1c
- Lipid panel (for triglyceride/HDL ratio)
The LabCorp Insulin Resistance Test Panel covers these essentials and is HSA/FSA eligible at approximately $89 — a reasonable cost for a comprehensive metabolic snapshot if you don’t have recent labs.
Fast for at least 8 hours before the draw. This is non-negotiable. Eating before the test invalidates both your glucose and your insulin values. A single cracker an hour before the draw will artificially suppress your HOMA-IR and give you a falsely reassuring result.
Morning draws are preferable. Cortisol and other hormones follow circadian patterns that influence insulin levels. For reproducibility, aim for a draw before 10 AM.

Category 3 — Continuous Glucose Monitoring (CGM)
CGMs — small sensors worn on the upper arm or abdomen — measure interstitial glucose continuously throughout the day. They were developed for people with type 1 and type 2 diabetes but have become increasingly accessible to people without diabetes who want to understand their glucose patterns.
What CGMs can tell you:
- How sharply your blood sugar spikes after specific foods
- How long it takes to return to baseline after a meal
- Whether you have nocturnal glucose fluctuations
What CGMs cannot tell you:
- Your fasting insulin level
- Your HOMA-IR
- Whether you have insulin resistance specifically (as opposed to impaired glucose regulation from other causes)
CGM is a behavioral tool. It shows you the effect, not the mechanism. A person with insulin resistance may have normal CGM patterns because their pancreas is still compensating with higher insulin output — the glucose looks fine, but the insulin doing the work is excessive. That’s precisely what HOMA-IR captures.
CGMs are most useful as a complement to blood testing, not a replacement for it.
The Free Starting Point: Calculate Your HOMA-IR Now
HOMA-IR (Homeostatic Model Assessment of Insulin Resistance) is a mathematical index derived from two fasting values: glucose and insulin. It was developed by Matthews and colleagues in 1985 and has since become the standard proxy measure for insulin resistance in large epidemiological studies.
Check the unit your lab uses — it appears right after the number on your results sheet: mg/dL or mmol/L. Select it above, enter your two values, and the calculator does the rest.
HOMA-IR insulin resistance calculator with unit toggle and TG/HDL ratio
Formula (mg/dL): (fasting insulin × fasting glucose) ÷ 405. For informational purposes only. Discuss your results with your healthcare provider.
How to Read Your HOMA-IR: What the Number Actually Means
This section is the clinical gap that no competitor currently fills adequately. Here is what the published literature and clinical practice converge on:
HOMA-IR | Interpretation |
|---|---|
< 1.0 | Excellent insulin sensitivity |
1.0 – 1.9 | Normal range for most non-diabetic adults |
2.0 – 2.9 | Early insulin resistance — warrants monitoring and lifestyle review |
≥ 3.0 | Significant insulin resistance — clinical attention indicated |
≥ 5.0 | Severe insulin resistance — strong association with pre-diabetes, metabolic syndrome, NAFLD |
What physicians know that most online guides don’t tell you:
The “normal” reference range varies by population. The cutoff of 2.0 is widely cited, but some studies place the threshold for significant insulin resistance at 2.5 or even 3.0 depending on the ethnic group studied and the reference laboratory. A HOMA-IR of 2.3 in a lean, active individual with no other metabolic risk factors is different from a HOMA-IR of 2.3 in someone with central obesity, elevated triglycerides, and fatigue after every meal.
A single number is not a diagnosis. HOMA-IR is a screening tool. It cannot distinguish between insulin resistance due to lifestyle factors versus secondary causes (certain medications, hormonal disorders, liver disease). If your HOMA-IR is elevated, the appropriate next step is a clinical evaluation — not a supplement purchase.
Serial measurements matter more than a single result. If you measure today and again in six months after dietary changes, the direction of change is more informative than any single absolute value. A HOMA-IR dropping from 3.8 to 2.1 is a meaningful metabolic improvement, regardless of whether the endpoint value is “normal.”
Fasting insulin is the variable that gets most distorted. Insulin is extremely sensitive to pre-analytical conditions — recent food intake, stress, intense exercise in the 24 hours before the draw. If your fasting insulin seems unexpectedly high or low, repeat the test under controlled conditions before drawing conclusions.
Other Markers That Signal Insulin Resistance
HOMA-IR is the most validated index, but it’s not the only signal in your bloodwork. These four additional markers, taken together, paint a more complete picture.
Fasting insulin alone. Even before calculating HOMA-IR, a fasting insulin above 10–12 µIU/mL in a non-diabetic adult is a flag worth discussing with a physician. Many patients have been told their glucose is “normal” for years while their insulin has been quietly climbing — a classic early-stage pattern.
HbA1c. This reflects your average blood glucose over the preceding 2–3 months. An HbA1c between 5.7% and 6.4% indicates pre-diabetes. Importantly, you can have insulin resistance with a completely normal HbA1c if your pancreas is still compensating adequately. HbA1c is a downstream marker; it becomes abnormal later in the process.
Triglycerides and HDL cholesterol. The triglyceride-to-HDL ratio is one of the most underappreciated markers in routine metabolic screening. Insulin resistance impairs the clearance of triglycerides from the bloodstream while simultaneously lowering HDL. A ratio above 3.0 (in mg/dL units) or above 1.3 (in mmol/L units) is associated with significant insulin resistance and is strongly predictive of cardiovascular risk.
If you already have a standard lipid panel from any recent blood test, this ratio is calculable today — no additional testing required.
Fasting glucose. A fasting glucose of 100–125 mg/dL (5.6–6.9 mmol/L) falls in the impaired fasting glucose range — not diabetes, but not optimal. Normal fasting glucose does not exclude insulin resistance, particularly in earlier stages.
Frequently Asked Questions
Can you self-test for insulin resistance?
Yes and no — and the distinction matters. You can perform a meaningful preliminary self-assessment using waist circumference, your existing lab values, and symptom patterns. If you have fasting glucose and fasting insulin from any recent blood test, you can calculate HOMA-IR yourself right now. What you cannot do at home is the gold-standard measurement — the hyperinsulinemic-euglycemic clamp — which requires hospital-level equipment and is used only in research settings. For practical purposes, HOMA-IR from a standard fasting blood draw is the best accessible proxy.
How do I check if I am insulin resistant?
Start with what you already have. Review any bloodwork from the past 12 months for fasting insulin and fasting glucose. If both are present, calculate your HOMA-IR using the calculator above. Check your waist circumference. Review the symptom patterns described in How to Tell If You Have Insulin Resistance — post-meal fatigue, afternoon energy crashes, difficulty losing abdominal weight, and carbohydrate cravings are common patterns. If multiple signals align, bring the question to your physician explicitly: ask for a fasting insulin test if it wasn’t previously ordered. described in How to Tell If You Have Insulin Resistance
What is a normal HOMA-IR score?
For most non-diabetic adults in published research, a HOMA-IR below 2.0 is considered within the normal range, with values below 1.0 reflecting excellent insulin sensitivity. The clinical threshold for “significant insulin resistance” is generally placed at 2.5–3.0 in most guideline documents, though this varies by population and reference laboratory. What matters as much as the absolute number is the full clinical picture: the same HOMA-IR value carries different meaning depending on your waist circumference, lipid profile, blood pressure, and symptom pattern.
What blood tests show insulin resistance?
No single blood test definitively diagnoses insulin resistance outside of a research setting. In clinical practice, the most informative combination is: fasting insulin + fasting glucose (to calculate HOMA-IR), HbA1c, and a lipid panel (for the triglyceride/HDL ratio). Of these, fasting insulin is the one most commonly omitted from routine panels and the most important to request specifically. If your physician hasn’t included it, ask directly: “Can you add a fasting insulin to my next metabolic workup?”
What to Do With Your Results
If your HOMA-IR is below 2.0 and your other markers are normal: You’re in a good metabolic position. The most useful thing you can do is establish a baseline to track against over time — especially if you have family history of type 2 diabetes or are approaching midlife, then you experienced 100% insulin resistance test at home.
If your HOMA-IR is between 2.0 and 3.0: This range warrants attention, not panic. It’s the zone where lifestyle changes have the strongest evidence for reversing the trend before it becomes a clinical diagnosis. The Diabetes Prevention Program trial demonstrated meaningful risk reduction through modest, sustainable changes. Your primary care physician should be aware of this result.
If your HOMA-IR is above 3.0: This is a clinical signal that deserves a proper medical evaluation. Elevated HOMA-IR at this level is associated with increased cardiovascular risk, NAFLD, and progression toward pre-diabetes. It’s not a reason to self-prescribe supplements — it’s a reason to have an informed conversation with your physician about what’s driving the resistance and what interventions are appropriate for your specific situation.
The Bottom Line
“Testing for insulin resistance at home” means three different things: truly at-home methods that require no purchase, order-online lab services that still require a blood draw, and wearable glucose monitors that track glucose patterns but not insulin resistance directly.
If you already have fasting glucose and fasting insulin values from any recent bloodwork, you can calculate your HOMA-IR today — no new test required. That’s your free starting point.
If you don’t have those values, a fasting blood panel that includes insulin, glucose, HbA1c, and lipids is the most clinically useful single test you can order. Whether that comes through your physician or a direct-access lab service is a practical decision — what matters is that you fast properly, draw in the morning, and have someone who can interpret the results in the context of your full picture.
Numbers without context are noise. Understanding what you’re measuring — and what it can and can’t tell you — is the only starting point worth having.
For a full explanation of what insulin resistance is and how it develops, see What Is Insulin Resistance? The Complete Guide. If you’re not sure whether to even get tested, the self-assessment in How to Tell If You Have Insulin Resistance is a useful first step.

— Dr. Nathan Wells, MD
Physician | 25+ years in clinical and pharmaceutical medicine
Take good care.
Want practical metabolic health insights, weekly? Get your free physician’s guide — “5 Signs You Have Insulin Resistance” — plus evidence-based clarity from a physician, straight to your inbox. → Subscribe to the SugarWiseLife weekly briefing
References
This article is for informational purposes only and does not constitute medical advice. The content on SugarWiseLife.com is intended to support, not replace, the relationship between you and your healthcare provider. Dr. Nathan Wells is a pen name used for privacy purposes. Nothing in this article should be used to diagnose or treat a medical condition. Always consult a qualified healthcare professional before making changes to your diet, exercise routine, or medication.
For full details, see our Medical Disclaimer, Editorial Policy, and Affiliate Disclosure.