Insulin Resistance and Hair Loss — When Your Body Sends the Same Signal Twice
There is a conversation I have had more times than I can count. A patient sits across from me, and I explain what insulin resistance does to the body — the fatigue, the weight, the cravings, and yes, sometimes the hair. I watch them absorb it. Then, months later, I start them on a GLP-1 medication, and I have to explain that the treatment may cause hair loss too. The same words. The same symptom. A different cause entirely.
That is the moment their brain freezes.
Insulin resistance and hair loss are connected — but not in the way most people assume. And when GLP-1 medications enter the picture, the confusion deepens. This article is here to untangle it, clearly and honestly, so you understand what is happening and why.
In this Article
Why Insulin Resistance and Hair Loss Are Connected
Your hair follicle is not a passive bystander. It is a metabolically active tissue — one of the most sensitive in the body to hormonal and inflammatory shifts. When insulin resistance takes hold, it sets off a chain of events that the follicle cannot ignore.
Here is the core mechanism. Insulin resistance drives chronically elevated insulin levels — a state called hyperinsulinemia. High insulin stimulates the ovaries (in women) and the adrenal glands to produce androgens, particularly testosterone and its more potent derivative, dihydrotestosterone (DHT). DHT is the molecule most directly responsible for androgenetic alopecia — pattern hair loss. It binds to receptors in genetically susceptible follicles, shortening the hair growth cycle until the follicle eventually miniaturizes and stops producing visible hair.
This is not a side effect of insulin resistance. It is a downstream consequence of the metabolic dysfunction itself.
There is a second mechanism at work: chronic low-grade inflammation. Insulin resistance maintains a persistent inflammatory state — elevated cytokines, oxidative stress, impaired microcirculation. The follicle sits in this inflammatory environment and suffers for it. Blood supply to the scalp diminishes. Follicle stem cells are disrupted. Growth cycles shorten.
The result is hair loss that arrives quietly, without drama, and is easy to attribute to stress, age, or genetics — when the real driver is metabolic.
For a fuller picture of what insulin resistance does to your metabolism, the complete guide is here.
It Looks Different in Women and Men
The same upstream cause — insulin resistance — expresses differently depending on your biology.
In women, the dominant pathway runs through androgen excess. Insulin resistance is the metabolic engine behind polycystic ovary syndrome (PCOS), the most common hormonal disorder in women of reproductive age. Elevated insulin drives androgen overproduction, which disrupts ovulation and produces the characteristic signs of PCOS — including diffuse hair thinning across the crown and top of the scalp. This is not the same pattern as male baldness. It is a widening part, a loss of density, a ponytail that feels thinner than it used to.
Women with insulin resistance who do not have a PCOS diagnosis may still experience androgen-driven hair thinning, particularly as estrogen declines around perimenopause — a period when insulin sensitivity also tends to worsen. The convergence of these two hormonal shifts can accelerate hair loss significantly. For a deeper look at how insulin resistance manifests differently in women across hormonal stages, the article on insulin resistance symptoms in women covers this in detail.
In men, the data is striking. A 2025 case-control study by Erden and colleagues found a significantly higher prevalence of insulin resistance and metabolic syndrome in young men with early-onset androgenetic alopecia — men losing hair in their twenties and thirties, well before the age when pattern baldness is typically expected. An earlier study by Swaroop and colleagues (2017) found associations between early-onset AGA and metabolic syndrome, though results on insulin resistance alone were mixed.
The clinical implication is important: in a young man presenting with premature hair loss, metabolic health deserves a place in the evaluation. The hairline may be the first visible signal of something systemic.
And Then the Treatment Does It Too
This is where patients look at me like I have said something impossible.
GLP-1 medications — semaglutide, tirzepatide — are among the most effective tools we have for treating insulin resistance and its metabolic consequences. They work. And in a meaningful proportion of patients, they cause hair loss.
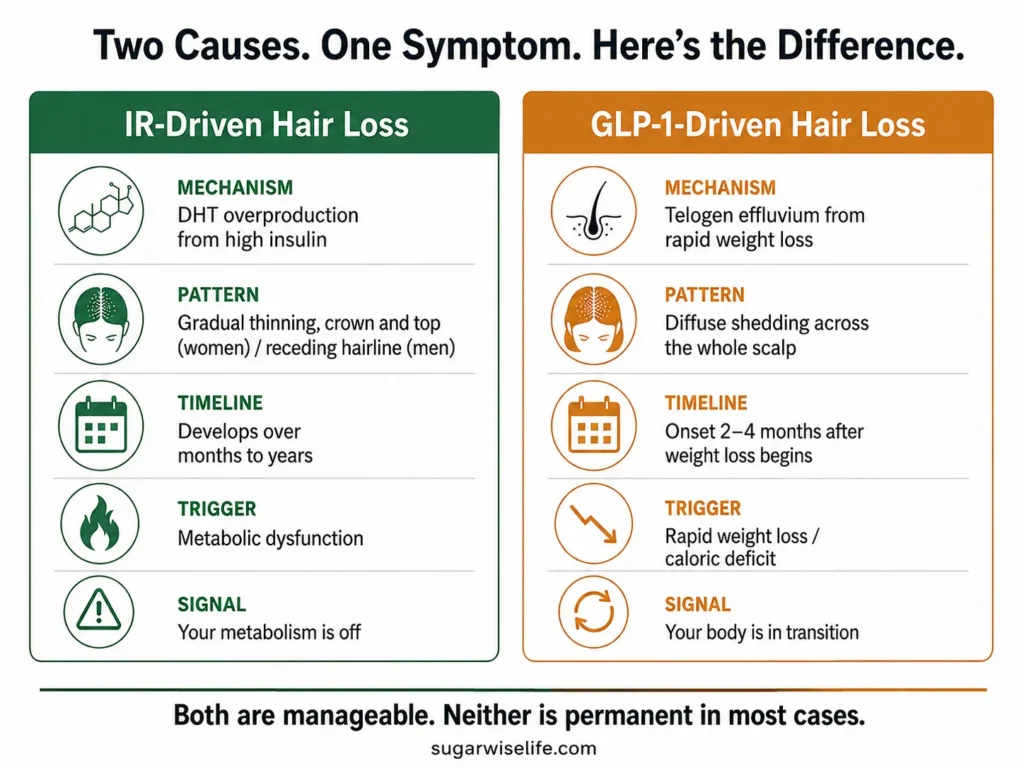
But it is a different kind of hair loss, driven by an entirely different mechanism.
GLP-1-associated hair loss is primarily telogen effluvium — a temporary, stress-induced shedding triggered by rapid weight loss. When the body loses weight quickly, the metabolic stress of that transition pushes a larger-than-normal proportion of hair follicles into the resting (telogen) phase simultaneously. Two to four months later, that hair sheds. The follicle is intact. The shedding is not permanent in most cases.
This is not DHT-mediated. This is not androgen-driven. It is the follicle’s response to physiological change — the same phenomenon seen after surgery, severe illness, or significant caloric restriction.
Same symptom. Different story.
The full mechanism, timeline, and management protocol for GLP-1-associated hair loss is covered in the dedicated article on GLP-1 medications and hair loss. If you are currently on a GLP-1 and experiencing shedding, that is the right place to start.
What matters here is the distinction: treating insulin resistance with GLP-1 medications may temporarily worsen the hair situation before it improves it. The IR-driven androgen excess resolves as metabolic health improves. The telogen effluvium passes. Understanding which phase you are in changes how you respond to it.
How to Tell Which Kind You Have
Not all hair loss looks the same. The pattern, timeline, and context offer meaningful clues.
If you are not on a GLP-1 and experiencing hair thinning alongside other signs of metabolic dysfunction — unexplained fatigue, difficulty losing weight, skin changes, blood sugar irregularities — insulin resistance deserves serious consideration as a contributing cause. The article on how to check whether you have insulin resistance walks through the practical steps.
If you are on a GLP-1 and experiencing shedding 2–4 months into treatment, telogen effluvium is the most likely explanation. Both can coexist.
What Actually Helps — Treating the Root
Here is the part that often surprises people: addressing insulin resistance is the most direct intervention for IR-driven hair loss. There is no topical treatment for hyperinsulinemia.
Lifestyle first. The interventions that improve insulin sensitivity — resistance training, reduced refined carbohydrate intake, adequate protein, sleep, stress management — also reduce the androgen excess that drives hair thinning. This is not a secondary benefit. It is the mechanism.
Nutritional support. Certain nutrients support follicle health and are commonly depleted in states of insulin resistance or rapid weight loss:
- Zinc — involved in hair follicle cycling and androgen metabolism. Deficiency is associated with hair loss. A serum zinc test before supplementing is worthwhile.
- Inositol — particularly myo-inositol, has shown benefit in PCOS-related androgen excess and insulin sensitivity. Evidence is accumulating.
- Iron — ferritin levels below 30 ng/mL are associated with hair shedding independent of anemia. Worth checking.
- Berberine — an insulin sensitizer with a growing evidence base, relevant for patients who cannot or prefer not to use pharmaceutical interventions.
Protein. During weight loss — especially rapid weight loss on a GLP-1 — protein intake is protective for hair. The target of 1.2–1.6g per kilogram of body weight is supported by available data. This is covered in detail in the pillar article on what insulin resistance actually does to your metabolism.
Patience. IR-driven hair loss improves as metabolic health improves. It does not reverse overnight. The follicle needs time to exit its suppressed state and re-enter the growth phase. Months, not weeks.
Frequently Asked Questions
Is insulin resistance hair loss reversible?
In most cases, yes — partially to significantly. When the underlying metabolic dysfunction is addressed and androgen levels normalize, the follicle can re-enter the growth cycle. Recovery is not guaranteed for follicles that have fully miniaturized, but meaningful improvement is achievable for most patients who intervene before advanced follicle loss.
What does hair loss from insulin resistance look like?
In women, it typically presents as diffuse thinning across the crown and top of the scalp — a widening part and reduced density rather than a receding hairline. In men, it follows the pattern of androgenetic alopecia: receding at the temples and thinning at the crown. Unlike GLP-1-related shedding, it develops gradually over months or years.
How to reverse hair thinning from insulin resistance?
The most effective approach targets the root cause: improving insulin sensitivity through resistance training, dietary changes, adequate sleep, and stress management. Nutritional support — zinc, inositol, iron, adequate protein — plays a supporting role. Berberine is a reasonable option for those seeking a non-pharmaceutical insulin sensitizer. Results take months and require consistency.
What are the warning signs of insulin resistance beyond hair loss?
Hair thinning is one of the quieter signals. More common early signs include post-meal fatigue, persistent hunger shortly after eating, abdominal weight gain, brain fog, and skin changes such as acanthosis nigricans (darkening in skin folds) or skin tags. A fasting insulin test is the most direct way to assess insulin resistance before it shows up on standard blood glucose panels.
Conclusion
The body speaks in symptoms. Hair loss is one of its more personal languages — visible, daily, impossible to ignore. When insulin resistance is the author, the message is metabolic: something upstream has shifted, and the follicle is downstream of it.
When GLP-1 treatment enters the picture and seems to repeat the message, it is not contradiction. It is two different conversations happening in sequence. The first is a disease signal. The second is a transition signal. Both resolve — at different timelines, through different mechanisms — when the root is addressed.
The signal becomes readable once you know what it is saying.
— Dr. Nathan Wells, MD
Physician | 25+ years in clinical and pharmaceutical medicine
Take good care.
References
- Erden O et al. Increased Prevalence of Insulin Resistance and Metabolic Syndrome in Men With Early-Onset Androgenetic Alopecia: A Case–Control Study. Journal of Cosmetic Dermatology. 2025.
- Swaroop MR et al. The Association of Metabolic Syndrome and Insulin Resistance in Early-Onset Androgenetic Alopecia in Males: A Case–Control Study. Indian Journal of Dermatology. 2017.
- Stefanadi EC et al. Metabolic syndrome and the skin: a more than superficial association. Diabetology & Metabolic Syndrome. 2018.
- Li M et al. Trends in insulin resistance: insights into mechanisms and therapeutic strategy. Signal Transduction and Targeted Therapy. 2022.
- Sánchez-Garrido MA, Tena-Sempere M. Metabolic dysfunction in polycystic ovary syndrome: Pathogenic role of androgen excess and potential therapeutic strategies. Molecular Metabolism. 2020.
Want practical metabolic health insights, weekly? No noise — just evidence-based clarity from a physician. → Subscribe to the SugarWiseLife weekly briefing
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. The content on SugarWiseLife.com is intended to support, not replace, the relationship between you and your healthcare provider. Dr. Nathan Wells is a pen name used for privacy purposes. Nothing in this article should be used to diagnose or treat a medical condition. Always consult a qualified healthcare professional before making changes to your diet, exercise routine, or medication.